Anda mungkin juga menyukai
- Clinical PresentationDokumen54 halamanClinical PresentationSêrâphîm HâdíBelum ada peringkat
- Final P - CapDokumen77 halamanFinal P - CapPopey MooreBelum ada peringkat
- Kırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisDokumen40 halamanKırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisAli FalihBelum ada peringkat
- Rheumatology LastDokumen54 halamanRheumatology LastAbdallah K. RamadanBelum ada peringkat
- Typhoid Fever PPT 30-3-10Dokumen97 halamanTyphoid Fever PPT 30-3-10Anonymous hYMWbA100% (1)
- PneumoniaDokumen26 halamanPneumonialovelots1234Belum ada peringkat
- Essential Facts in Geriatric MedicineDokumen26 halamanEssential Facts in Geriatric MedicineDastan HadiBelum ada peringkat
- Polio EpidDokumen61 halamanPolio EpidLuthfi HakimBelum ada peringkat
- Hyperemesis GravidarumDokumen31 halamanHyperemesis GravidarumDastan HadiBelum ada peringkat
- PCAP Report ClerkshipDokumen54 halamanPCAP Report ClerkshipMichelleAquinoSuzukiBelum ada peringkat
- Knust Lect Infectious Disease IDokumen8 halamanKnust Lect Infectious Disease IAnastasiafynnBelum ada peringkat
- Viral ExanthemDokumen60 halamanViral ExanthemClaire GuanteroBelum ada peringkat
- Acute Poliomyelitis: BY: Reojano, Jeriby R. Paroginog, CharisDokumen35 halamanAcute Poliomyelitis: BY: Reojano, Jeriby R. Paroginog, CharisMarivic DianoBelum ada peringkat
- RNA Non Enveloped VirusesDokumen35 halamanRNA Non Enveloped VirusesRPh Krishna Chandra JagritBelum ada peringkat
- IM, CMV and Toxoplasma InfectionsDokumen112 halamanIM, CMV and Toxoplasma Infectionsnada9tarek-2Belum ada peringkat
- Infectious MononucleosisDokumen23 halamanInfectious Mononucleosis180045Belum ada peringkat
- Lecture 8 - PicornavirusesDokumen21 halamanLecture 8 - PicornavirusesJeanPaule JoumaaBelum ada peringkat
- Inf MononucleosysDokumen46 halamanInf MononucleosysStefan MarinBelum ada peringkat
- W1 L2 PneumoniaDokumen57 halamanW1 L2 PneumoniaAnas FikriBelum ada peringkat
- Infection PICU 1Dokumen33 halamanInfection PICU 1Mohamed ElgayarBelum ada peringkat
- Https://ar - scribd.com/document/391648283/OET Future Land Full Book Final Edition July 2018Dokumen52 halamanHttps://ar - scribd.com/document/391648283/OET Future Land Full Book Final Edition July 2018Qutaiba ShdaifatBelum ada peringkat
- CURA Mono, Rheu, HyperDokumen89 halamanCURA Mono, Rheu, Hyperwiwi_13Belum ada peringkat
- Infections of The Central Nervous System: DR John Egbagba FmcpathDokumen46 halamanInfections of The Central Nervous System: DR John Egbagba FmcpathPrincewill SeiyefaBelum ada peringkat
- Common Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorDokumen52 halamanCommon Viral Exanthemas (Measles, Chickenpox & Rubella) : DR Sarika Gupta (MD, PHD), Assistant ProfessorashighaBelum ada peringkat
- Lower Respiratory Tract InfectionDokumen21 halamanLower Respiratory Tract InfectionJohn Vincent Dy OcampoBelum ada peringkat
- Neonatal Sepsis 1219225703095484 9Dokumen50 halamanNeonatal Sepsis 1219225703095484 9Ali FalihBelum ada peringkat
- Chapter 1Dokumen30 halamanChapter 1Ayro Business CenterBelum ada peringkat
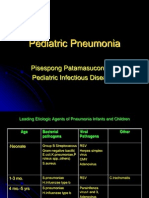
- Pediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesDokumen39 halamanPediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesSi PuputBelum ada peringkat
- Clinico-Pathologic Conference OutputDokumen3 halamanClinico-Pathologic Conference OutputNorman Vryne CaduaBelum ada peringkat
- Pneumonia - Dr. IonescuDokumen51 halamanPneumonia - Dr. IonescuArleen MatincaBelum ada peringkat
- Himanshu Gupta TaskDokumen5 halamanHimanshu Gupta TaskHimanshuBelum ada peringkat
- Pneumonia, BronchiolitisDokumen65 halamanPneumonia, BronchiolitisYemata HailuBelum ada peringkat
- Blok 27 PertussisDokumen36 halamanBlok 27 PertussisNiaaAprilita100% (1)
- Topic 2. Dyspnea. Complecated Pneumonia in Children. - ShortDokumen69 halamanTopic 2. Dyspnea. Complecated Pneumonia in Children. - ShortIbtissame BadadBelum ada peringkat
- A Case Presentation On PneumoniaDokumen74 halamanA Case Presentation On PneumoniaYengkhom YoshiBelum ada peringkat
- Diseases PIDSRDokumen25 halamanDiseases PIDSRaringkinking100% (1)
- "Neonatal Infections" Lecture 1: Pediatrics Dr. Sawsan AliDokumen5 halaman"Neonatal Infections" Lecture 1: Pediatrics Dr. Sawsan AliAmmarBelum ada peringkat
- Respiratory SystemDokumen30 halamanRespiratory SystemHani El-asferBelum ada peringkat
- Paramyxoviruses: Dr. Muna M A Yousif M.D Clinical MicrobiologyDokumen30 halamanParamyxoviruses: Dr. Muna M A Yousif M.D Clinical MicrobiologyJaydee PlataBelum ada peringkat
- PoliomyelitesDokumen35 halamanPoliomyelitesped medBelum ada peringkat
- Vaccine PreventableDokumen89 halamanVaccine PreventableMohammad Doctor CabdiraxmanBelum ada peringkat
- Neonatal SepsisDokumen5 halamanNeonatal SepsisBhawna PandhuBelum ada peringkat
- Lec 7 Infectious MononucleosisDokumen6 halamanLec 7 Infectious MononucleosisZizou ZidaneBelum ada peringkat
- GFDFDFDokumen7 halamanGFDFDFRm98Belum ada peringkat
- Patho Unit 5Dokumen37 halamanPatho Unit 5Shafiya ShaikBelum ada peringkat
- Hiv AidsDokumen7 halamanHiv Aidsandirio7486Belum ada peringkat
- Pneumonia: Presented By: DR Aakrit Dahal Intern, Shree Birendra Hospital Department of PaediatricsDokumen65 halamanPneumonia: Presented By: DR Aakrit Dahal Intern, Shree Birendra Hospital Department of PaediatricsAkrit DahalBelum ada peringkat
- Infectious Mononucleosis QSHDokumen15 halamanInfectious Mononucleosis QSH180045Belum ada peringkat
- HIV PediatricsDokumen15 halamanHIV Pediatricshussain AltaherBelum ada peringkat
- M Pneumoniae,: Community-Acquired PneumoniaDokumen3 halamanM Pneumoniae,: Community-Acquired PneumoniaOlaru CatalinaBelum ada peringkat
- Arv 13Dokumen97 halamanArv 13Matin Ahmad KhanBelum ada peringkat
- Polio 150416150654 Conversion Gate01Dokumen35 halamanPolio 150416150654 Conversion Gate01Bheru Lal0% (1)
- Pyrexia of Unknown OriginDokumen81 halamanPyrexia of Unknown OriginJithin Bhagavati Kalam100% (1)
- Infections of The Digestive GlandsDokumen17 halamanInfections of The Digestive GlandsCrystal Lynn Keener SciariniBelum ada peringkat
- The GI Viruses: Enteroviruses, Rotavirus and CalicivirusesDokumen58 halamanThe GI Viruses: Enteroviruses, Rotavirus and CalicivirusesQurban AliBelum ada peringkat
- The Wheezing Infant: Airway Problems in ChildrenDokumen4 halamanThe Wheezing Infant: Airway Problems in ChildrenDenise DelaneyBelum ada peringkat
- Immunology 8Dokumen37 halamanImmunology 8ukashazam19Belum ada peringkat
- Peds InfectiousDokumen8 halamanPeds InfectiousMohammad RammalBelum ada peringkat
- Infectious Diseases: A Geographic GuideDari EverandInfectious Diseases: A Geographic GuideEskild PetersenBelum ada peringkat
- A Patient Experience Course Syllabus: Integrating Service Sciences Research To Enhance Health-Care DeliveryDokumen5 halamanA Patient Experience Course Syllabus: Integrating Service Sciences Research To Enhance Health-Care DeliveryDastan HadiBelum ada peringkat
- Global Catastrophic Risks 2017 BWDokumen67 halamanGlobal Catastrophic Risks 2017 BWDastan HadiBelum ada peringkat
- Bo Pyawe PutekanDokumen73 halamanBo Pyawe PutekanDastan HadiBelum ada peringkat
- Diagnostic FaciesDokumen3 halamanDiagnostic FaciesDastan HadiBelum ada peringkat