Anda mungkin juga menyukai
- Hospital LiabilityDokumen12 halamanHospital LiabilityBlissy S. ItomBelum ada peringkat
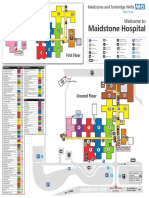
- Maidstone Hospital Internal MapDokumen1 halamanMaidstone Hospital Internal MapMwa0% (3)
- Letter Sent To Wellstar Health SystemDokumen4 halamanLetter Sent To Wellstar Health SystemLindsey BasyeBelum ada peringkat
- Er SopDokumen19 halamanEr Sopjaybeeclaire67% (3)
- US Healthcare System Analysis v2-0Dokumen31 halamanUS Healthcare System Analysis v2-0Achintya KumarBelum ada peringkat
- A History of NHS PrivatisationDokumen16 halamanA History of NHS PrivatisationProtect our NHSBelum ada peringkat
- Hospital Safety PromotionDokumen46 halamanHospital Safety PromotionRhodora BenipayoBelum ada peringkat
- NMC SVMH Presentation 7Mar2012Final-2Dokumen37 halamanNMC SVMH Presentation 7Mar2012Final-2dram408Belum ada peringkat
- Payment PDFDokumen35 halamanPayment PDFLauraMariaAndresanBelum ada peringkat
- ASNCH Letter To Mayor JohnsonDokumen2 halamanASNCH Letter To Mayor JohnsonRobert GarciaBelum ada peringkat
- NHS A4Dokumen2 halamanNHS A4Bronwen HandysideBelum ada peringkat
- Subject: Formal Complaint Against OACCAC Sent Via Mail and EmailDokumen3 halamanSubject: Formal Complaint Against OACCAC Sent Via Mail and Emailapi-88872975Belum ada peringkat
- Philippine Alliance of Patient Organization StatementDokumen2 halamanPhilippine Alliance of Patient Organization StatementJess LorenzoBelum ada peringkat
- Sample 5Dokumen7 halamanSample 5Nguyễn Thị ThờiBelum ada peringkat
- Brief Home Care Bill 175 Submission June 2020-06-15Dokumen12 halamanBrief Home Care Bill 175 Submission June 2020-06-15Doug Allan100% (1)
- Unite Guide To: Privatisation of The NHS EnglandDokumen24 halamanUnite Guide To: Privatisation of The NHS EnglandKarishma MartiniBelum ada peringkat
- Senate Hearing, 114TH Congress - Testimony On Rural HealthDokumen73 halamanSenate Hearing, 114TH Congress - Testimony On Rural HealthScribd Government DocsBelum ada peringkat
- AHA Statement Re ACOsDokumen24 halamanAHA Statement Re ACOsMSH_JD_CPABelum ada peringkat
- Paths To Prosperity: Patient-Centred Health CareDokumen16 halamanPaths To Prosperity: Patient-Centred Health CareDoug AllanBelum ada peringkat
- Listen All: Perspectives Regarding HomeDokumen1 halamanListen All: Perspectives Regarding Homeapi-88872975Belum ada peringkat
- Cecba Reform Group Media Release 25oct2015Dokumen3 halamanCecba Reform Group Media Release 25oct2015api-288922611Belum ada peringkat
- O'neill Report Reveals That Abbott's Health System Will Be A DisasterDokumen2 halamanO'neill Report Reveals That Abbott's Health System Will Be A DisasterannecharltonBelum ada peringkat
- Hospital Governance and Accountability in OntarioDokumen63 halamanHospital Governance and Accountability in OntarioNi Putu Sri wahyuniBelum ada peringkat
- Business Health Care Policy PaperDokumen7 halamanBusiness Health Care Policy Paperapi-272534722Belum ada peringkat
- Employee RelationsDokumen42 halamanEmployee RelationsGupta GauravBelum ada peringkat
- 2014-06-01 1030 VA Press Conference REMARKSDokumen2 halaman2014-06-01 1030 VA Press Conference REMARKSsenatortesterBelum ada peringkat
- Exorcising PhilHealth GhostsDokumen4 halamanExorcising PhilHealth GhostsArielBelum ada peringkat
- The Long Series of Failures of Private Clinics in Ontario: Hamilton SpectatorDokumen5 halamanThe Long Series of Failures of Private Clinics in Ontario: Hamilton Spectatorapi-345750272Belum ada peringkat
- Redford's ResponseDokumen5 halamanRedford's ResponsepkGlobalBelum ada peringkat
- SorbaraDokumen3 halamanSorbara404 System ErrorBelum ada peringkat
- Letter To Editor - Globe and Mail - June 11, 2012 Admin vs. CareDokumen1 halamanLetter To Editor - Globe and Mail - June 11, 2012 Admin vs. Careapi-88872975Belum ada peringkat
- Victoria Hospital Resdesign InitiativeDokumen6 halamanVictoria Hospital Resdesign InitiativeFatima Ajmal100% (1)
- Press Conference On The Release of NHI and The Medical Schemes Bills - 21 June 2018 - Medical Schemes Amendment BillDokumen9 halamanPress Conference On The Release of NHI and The Medical Schemes Bills - 21 June 2018 - Medical Schemes Amendment BillGemma RitchieBelum ada peringkat
- OD Apr15 CorporateLaws V2Dokumen3 halamanOD Apr15 CorporateLaws V2Chandra ClarkBelum ada peringkat
- The State of Government Owned Community HospitalsDokumen48 halamanThe State of Government Owned Community HospitalsAlex KacikBelum ada peringkat
- South Zone ED Phys Letter To MinisterDokumen4 halamanSouth Zone ED Phys Letter To MinisterCTV CalgaryBelum ada peringkat
- Ballad Health Comment Submission 8-2-19Dokumen21 halamanBallad Health Comment Submission 8-2-19Anonymous COFJlahBelum ada peringkat
- LHIN GraphicsDokumen2 halamanLHIN GraphicsThe Hamilton SpectatorBelum ada peringkat
- Ontario ChartDokumen7 halamanOntario ChartmichelestackarukBelum ada peringkat
- Rinah GrahamDokumen2 halamanRinah Grahameva agustinaBelum ada peringkat
- Expanded Pay For Doctors Amidst The PandemicDokumen1 halamanExpanded Pay For Doctors Amidst The PandemicDavid Josh AzueloBelum ada peringkat
- State of The County 2010Dokumen16 halamanState of The County 2010Daily FreemanBelum ada peringkat
- HealthcarepolicypaperDokumen6 halamanHealthcarepolicypaperapi-296425490Belum ada peringkat
- Letter To CMSDokumen7 halamanLetter To CMSWill SmithBelum ada peringkat
- Doug Ford Letter To Ontario Hospital CEOsDokumen5 halamanDoug Ford Letter To Ontario Hospital CEOsSunny CynthiaBelum ada peringkat
- Deccan Herald ArticleDokumen1 halamanDeccan Herald ArticleRajan DubeyBelum ada peringkat
- Jnma00789 0016Dokumen5 halamanJnma00789 0016mswBelum ada peringkat
- 4HE, - 3PIN: /-"5$3-!. 2%0/24 !ndrï - Arin /mbudsman of /ntario S UlyDokumen44 halaman4HE, - 3PIN: /-"5$3-!. 2%0/24 !ndrï - Arin /mbudsman of /ntario S UlyPatrick FafardBelum ada peringkat
- Insolvency For NHS Care Providers SubmissionDokumen1 halamanInsolvency For NHS Care Providers SubmissionWilliam WetherellBelum ada peringkat
- PO Box 64998 - St. Paul, MN - 55164-0998 - An Equal Opportunity and Veteran-Friendly EmployerDokumen10 halamanPO Box 64998 - St. Paul, MN - 55164-0998 - An Equal Opportunity and Veteran-Friendly EmployerBob HumeBelum ada peringkat
- Improving Healthcare Services at Reduced PricesDokumen5 halamanImproving Healthcare Services at Reduced PricesAshwani RanaBelum ada peringkat
- SEIU-UHW's Dishonest "Open Letter" Regarding Withdrawal of California Ballot Initiative, Sacramento Bee: June 30, 2016Dokumen1 halamanSEIU-UHW's Dishonest "Open Letter" Regarding Withdrawal of California Ballot Initiative, Sacramento Bee: June 30, 2016Anonymous iC9QziK0% (1)
- Case BackgroundDokumen3 halamanCase BackgroundPrasasti Chandra AbadiBelum ada peringkat
- DR Naffah On ObamacareDokumen1 halamanDR Naffah On ObamacarePaul Conner50% (6)
- Bureaucracy: Life CycleDokumen2 halamanBureaucracy: Life CycleMarlon VentulanBelum ada peringkat
- Middlebury Health District ReportDokumen5 halamanMiddlebury Health District ReportRepublican-AmericanBelum ada peringkat
- Selling Our Souls: The Commodification of Hospital Care in the United StatesDari EverandSelling Our Souls: The Commodification of Hospital Care in the United StatesBelum ada peringkat
- External Review of London Emergency Dept.Dokumen11 halamanExternal Review of London Emergency Dept.The London Free PressBelum ada peringkat
- Canada: Robert G. Evans University of British ColumbiaDokumen10 halamanCanada: Robert G. Evans University of British ColumbiaDylan MartinezBelum ada peringkat
- Nhif BoardDokumen4 halamanNhif BoardDennis ItumbiBelum ada peringkat
- NgocTrinh - Public HealthDokumen2 halamanNgocTrinh - Public HealthPhương NguyênBelum ada peringkat
- Textbook of Urgent Care Management: Chapter 33, EMTALA in Urgent Care MedicineDari EverandTextbook of Urgent Care Management: Chapter 33, EMTALA in Urgent Care MedicineBelum ada peringkat
- Canadian Health Care Blueprint: Reaching Higher, Working Smarter. Getting StrongerDari EverandCanadian Health Care Blueprint: Reaching Higher, Working Smarter. Getting StrongerBelum ada peringkat
- Running Head: Delegations and Lessons 1Dokumen5 halamanRunning Head: Delegations and Lessons 1StephanieBelum ada peringkat
- More Than Freedom: By: Brent Marco M. Camus, Daphnie Paulynne Santos, Jermeign GonzalesDokumen43 halamanMore Than Freedom: By: Brent Marco M. Camus, Daphnie Paulynne Santos, Jermeign GonzalesJ GAMEZBelum ada peringkat
- January 23 2015 PDFDokumen39 halamanJanuary 23 2015 PDFfijitimescanadaBelum ada peringkat
- Waiver For Turkey TrotDokumen1 halamanWaiver For Turkey Trotapi-85191986Belum ada peringkat
- SW 5720 Final PPDokumen12 halamanSW 5720 Final PPapi-251722980Belum ada peringkat
- Cheryl Lynn RomeroDokumen2 halamanCheryl Lynn RomeroEric RobertsonBelum ada peringkat
- Inspector General ReportDokumen48 halamanInspector General ReportDenise PridgenBelum ada peringkat
- Chapter 4 INTERNAL ENVIRONMENTAL ANALYSIS COMPETITIVE ADVANTAGEDokumen18 halamanChapter 4 INTERNAL ENVIRONMENTAL ANALYSIS COMPETITIVE ADVANTAGESheeza AsharBelum ada peringkat
- Unit 2 TV Documentary:: Summit 2 Video ScriptDokumen2 halamanUnit 2 TV Documentary:: Summit 2 Video ScriptRafael SaraviaBelum ada peringkat
- Body Weakness NCPDokumen1 halamanBody Weakness NCPtwicetrashBelum ada peringkat
- Registration of Patient Transport VehicleDokumen2 halamanRegistration of Patient Transport VehicleMenGuitar100% (1)
- NEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0Dokumen1 halamanNEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0Ivoria Septiani GuloBelum ada peringkat
- Philippines Report 2008 Price Components Pricing SurveysDokumen60 halamanPhilippines Report 2008 Price Components Pricing SurveysJoannie Galarosa PalacioBelum ada peringkat
- Problems and Solutions: Revision Questions in Undergraduate SurgeryDokumen13 halamanProblems and Solutions: Revision Questions in Undergraduate Surgerytamikanji100% (1)
- Diagnosis of Decreased Hemisphericity by AK Muscle Testing-ICAKDokumen39 halamanDiagnosis of Decreased Hemisphericity by AK Muscle Testing-ICAKJohn de CogBelum ada peringkat
- Republic Act No. 6615, (1972-10-23)Dokumen3 halamanRepublic Act No. 6615, (1972-10-23)MiakaBelum ada peringkat
- From Operasi Celah Bibir Yayasan Vivitas-Converted - EDIT ISIDokumen10 halamanFrom Operasi Celah Bibir Yayasan Vivitas-Converted - EDIT ISIBagusBhudiBhaktiBelum ada peringkat
- Strategies To Enhance Adoption of Ventilator-Associated Pneumonia Prevention Interventions A Systematic Literature ReviewDokumen8 halamanStrategies To Enhance Adoption of Ventilator-Associated Pneumonia Prevention Interventions A Systematic Literature ReviewRoberto Linhares de FreitasBelum ada peringkat
- Vascular Disorders of The Posterior Circulation - An Anatomico-Clinical OverviewDokumen3 halamanVascular Disorders of The Posterior Circulation - An Anatomico-Clinical OverviewSagar GopaniBelum ada peringkat
- NMHPDokumen3 halamanNMHPJis Johnson P PBelum ada peringkat
- Alat HectingDokumen4 halamanAlat HectingjuliperBelum ada peringkat
- WUK 2011 - 7 Jackie Haynes Rosie Callaghan Properties of Honey Its Mode of Action and Clinical Outcomes - 3Dokumen7 halamanWUK 2011 - 7 Jackie Haynes Rosie Callaghan Properties of Honey Its Mode of Action and Clinical Outcomes - 3Elvis OgbeBelum ada peringkat
- Rdav ResumeDokumen1 halamanRdav Resumeapi-383799988Belum ada peringkat
- February 7, 2014 Strathmore TimesDokumen28 halamanFebruary 7, 2014 Strathmore TimesStrathmore TimesBelum ada peringkat
- Importance of Support ServicesDokumen5 halamanImportance of Support ServicesRockson Ohene AsanteBelum ada peringkat
- Slow, Low, Efficient, Daily Dialysis (SLEDD) in The Critically Ill PatientDokumen1 halamanSlow, Low, Efficient, Daily Dialysis (SLEDD) in The Critically Ill PatientarisyiBelum ada peringkat