Anda mungkin juga menyukai
- AlHawasi - Manual of Clinical PediatricDokumen276 halamanAlHawasi - Manual of Clinical PediatricAhmad Just100% (2)
- The Strength of The Fading and Dancing ArgumentsDokumen50 halamanThe Strength of The Fading and Dancing ArgumentsPhil SpitzerBelum ada peringkat
- Elevations RTC InvestigationsDokumen77 halamanElevations RTC InvestigationsTTILawBelum ada peringkat
- Paradox of Self-Conciousness, The - BermúdezDokumen17 halamanParadox of Self-Conciousness, The - Bermúdezgheorghe3Belum ada peringkat
- Review The Art of Philosophy Wisdom As A PracticeDokumen3 halamanReview The Art of Philosophy Wisdom As A PracticeMatiasBarrios86Belum ada peringkat
- Aristotle's Take On Socratic ParadoxDokumen154 halamanAristotle's Take On Socratic ParadoxFlorz GelarzBelum ada peringkat
- Personal Construct Theory As A Line of InferenceDokumen9 halamanPersonal Construct Theory As A Line of InferenceJosh SofferBelum ada peringkat
- DG Bell - Henry Alline and Maritime ReligionDokumen30 halamanDG Bell - Henry Alline and Maritime ReligionChris SchelinBelum ada peringkat
- Charlotte Radler - Detachment in Meister EckhartDokumen8 halamanCharlotte Radler - Detachment in Meister EckhartChris SchelinBelum ada peringkat
- In love I am more GodDokumen29 halamanIn love I am more GodChris SchelinBelum ada peringkat
- Joseph Wong - The Jesus Prayer and Inner StillnessDokumen14 halamanJoseph Wong - The Jesus Prayer and Inner StillnessChris Schelin100% (3)
- 09 ITLS PretestDokumen6 halaman09 ITLS PretestArlanosaurus100% (2)
- Ranger Medic Handbook 2007Dokumen154 halamanRanger Medic Handbook 2007Jared A. Lang93% (15)
- U1L7 Student GuideDokumen4 halamanU1L7 Student Guideria wu100% (3)
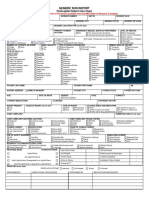
- Run Report Generic TemplateDokumen2 halamanRun Report Generic TemplatemeljamerlanBelum ada peringkat
- Exam1 100731100921 Phpapp02Dokumen34 halamanExam1 100731100921 Phpapp02Yaj CruzadaBelum ada peringkat
- Consciousness Origins of PDFDokumen6 halamanConsciousness Origins of PDF11111Belum ada peringkat
- THE STRANGELOOP OF METAPHYSICAL MODELSDokumen2 halamanTHE STRANGELOOP OF METAPHYSICAL MODELSRadu AnghelBelum ada peringkat
- Theory of Paradoxes and Contradictory Rule Sets Sujay Rao MandavilliDokumen8 halamanTheory of Paradoxes and Contradictory Rule Sets Sujay Rao MandavilliSujay Rao MandavilliBelum ada peringkat
- Paradoxes of MindfulnessDokumen9 halamanParadoxes of MindfulnessSHEIKH MOHAMMAD ASIF 2071021Belum ada peringkat
- Resolving Paradoxes - Issue 106 - Philosophy NowDokumen5 halamanResolving Paradoxes - Issue 106 - Philosophy NowBanderlei SilvaBelum ada peringkat
- Paradoxes ExplainedDokumen13 halamanParadoxes ExplainedHussein SarrarBelum ada peringkat
- Near-Death Experiences in Ancient Greek PhilosophyDokumen9 halamanNear-Death Experiences in Ancient Greek PhilosophyIvan PavlovBelum ada peringkat
- Paradox of Life - 001Dokumen12 halamanParadox of Life - 001Gim ReyesBelum ada peringkat
- NDE Provides Evidence of Veridical OBE and HealingDokumen16 halamanNDE Provides Evidence of Veridical OBE and HealingNus EuBelum ada peringkat
- Thresholds of AwarenessDokumen14 halamanThresholds of AwarenessLucian DantesBelum ada peringkat
- Near-Death Experiences More Vivid Than Real LifeDokumen3 halamanNear-Death Experiences More Vivid Than Real LifefuturistscribdBelum ada peringkat
- Mysteries of Knowledge Beyond Our SensesDokumen3 halamanMysteries of Knowledge Beyond Our Senseslil telBelum ada peringkat
- Sartori FenwickDokumen16 halamanSartori FenwickjuanportoBelum ada peringkat
- Glauco Schaffer Near Death ExperienceDokumen6 halamanGlauco Schaffer Near Death Experienceglaucolimo100% (1)
- Paradoxes and Self-Reference in W.V. Quine's "The Ways of ParadoxDokumen9 halamanParadoxes and Self-Reference in W.V. Quine's "The Ways of ParadoxSoumya DuttsBelum ada peringkat
- Continuity of Consciousness After DeathDokumen42 halamanContinuity of Consciousness After Deathdick_henriqueBelum ada peringkat
- There Is Nothing Paranormal About Near-Death PDFDokumen3 halamanThere Is Nothing Paranormal About Near-Death PDFMohammad Al-SalehBelum ada peringkat
- Experiential access to other minds: Three models comparedDokumen18 halamanExperiential access to other minds: Three models comparedorlando garcia100% (1)
- Near Life Queer DeathDokumen20 halamanNear Life Queer DeathCait LynnBelum ada peringkat
- Inflammatory Breast CancerDokumen6 halamanInflammatory Breast CancerHafsa ShafiqueBelum ada peringkat
- Greene Journal of Near Death Studies - 1999!17!151 191Dokumen41 halamanGreene Journal of Near Death Studies - 1999!17!151 191360DBelum ada peringkat
- Eckhart FinalDokumen20 halamanEckhart FinalcdcrossroaderBelum ada peringkat
- Consciousness and Self-ConsciousnessDokumen21 halamanConsciousness and Self-Consciousnessantonio_ponce_1Belum ada peringkat
- Cosmogony of ReasonDokumen15 halamanCosmogony of ReasonСергей КлевцовBelum ada peringkat
- Canullo, Carla, "Michel Henry: From The Essence of Manifestation To The Essence of Religion"Dokumen10 halamanCanullo, Carla, "Michel Henry: From The Essence of Manifestation To The Essence of Religion"Micaela SzeftelBelum ada peringkat
- Modern Neuroscience and Near-Death Experiences Expectancies and ImplicationsDokumen7 halamanModern Neuroscience and Near-Death Experiences Expectancies and ImplicationsNicky KellyBelum ada peringkat
- Consciousness: Awareness Attention Selective Attention Divided Attention Dichotic ListeningDokumen11 halamanConsciousness: Awareness Attention Selective Attention Divided Attention Dichotic Listeningvishnur795Belum ada peringkat
- Consciousness and Minimal Selfhood Getti PDFDokumen19 halamanConsciousness and Minimal Selfhood Getti PDFRobson BarcelosBelum ada peringkat
- Publications On Psi Research (Dean Radin)Dokumen8 halamanPublications On Psi Research (Dean Radin)Frater T.A.S.Belum ada peringkat
- One's Dharma Practice: The Wisdom in DirectingDokumen9 halamanOne's Dharma Practice: The Wisdom in DirectingDudjomBuddhistAssoBelum ada peringkat
- Sociology, Understanding and Changing The Social WorldDokumen1.000 halamanSociology, Understanding and Changing The Social WorldSOHATEEBelum ada peringkat
- NICOLESCU The Idea of Levels of Reality and It Relevance For Non-Reduction and PersonhoodDokumen13 halamanNICOLESCU The Idea of Levels of Reality and It Relevance For Non-Reduction and PersonhoodDavid García DíazBelum ada peringkat
- Integral Semiotics: Understanding Linguistic MeaningDokumen45 halamanIntegral Semiotics: Understanding Linguistic MeaningPallab ChakrabortyBelum ada peringkat
- Bell - Deleuze, Realism, AntirealismDokumen17 halamanBell - Deleuze, Realism, AntirealismoforikoueBelum ada peringkat
- Akiwowo - Sociology in Africa TodayDokumen72 halamanAkiwowo - Sociology in Africa TodayViviane Pereira100% (2)
- The Reality of Free WillDokumen16 halamanThe Reality of Free WillClaus JanewBelum ada peringkat
- 3 Esoteric Life ViewDokumen97 halaman3 Esoteric Life ViewSimon EarthMan BarjonaBelum ada peringkat
- Transdisciplinarity Building Bridges Between Fields of Knowledge, Facts, People, CulturesDokumen43 halamanTransdisciplinarity Building Bridges Between Fields of Knowledge, Facts, People, CulturesRoland AdorjaniBelum ada peringkat
- Death and Dying in The Tibetan TraditionDokumen13 halamanDeath and Dying in The Tibetan TraditionchrifotiBelum ada peringkat
- Nde Aftereffects CourseDokumen51 halamanNde Aftereffects Courseapi-308577129Belum ada peringkat
- Perspectiva fenomenológica del cuerpo que danza (39Dokumen15 halamanPerspectiva fenomenológica del cuerpo que danza (39Ruben Dario Luna RLBelum ada peringkat
- Edmund Husserl's Phenomenology: The Principle of Intentionality and The Methods of Reduction Key WordsDokumen10 halamanEdmund Husserl's Phenomenology: The Principle of Intentionality and The Methods of Reduction Key Wordsmt_tejaBelum ada peringkat
- Why the Paradox Mindset is Key to CreativityDokumen4 halamanWhy the Paradox Mindset is Key to CreativityAnna MayerBelum ada peringkat
- Duality and Nonduality in Systems TheoryDokumen18 halamanDuality and Nonduality in Systems TheoryvitazzoBelum ada peringkat
- Critique of Berkeley's IdealismDokumen8 halamanCritique of Berkeley's IdealismPaul HorriganBelum ada peringkat
- Debating Humanity. Towards A Philosophical Sociology: Daniel CherniloDokumen20 halamanDebating Humanity. Towards A Philosophical Sociology: Daniel CherniloEka Wahyudi NggoheleBelum ada peringkat
- Epistemology: An Informal Look at Theories of KnowledgeDokumen31 halamanEpistemology: An Informal Look at Theories of KnowledgeKristoff Dalumpines CabilaBelum ada peringkat
- Intentionality NotesDokumen22 halamanIntentionality Notesshirley_hu_15Belum ada peringkat
- The Real Self According to J. Dashiell StoopsDokumen11 halamanThe Real Self According to J. Dashiell StoopsDharylle CariñoBelum ada peringkat
- Wittgenstein's Refutation of IdealismDokumen32 halamanWittgenstein's Refutation of IdealismFaiz AlamBelum ada peringkat
- Searle ConscUnconsc&Intentionality 1991 OCR PDFDokumen22 halamanSearle ConscUnconsc&Intentionality 1991 OCR PDFStephen RowntreeBelum ada peringkat
- IntentionalityDokumen28 halamanIntentionalityCarlo Emmanuel DyBelum ada peringkat
- The Journal For Baptist Theology and Ministry - Spring 2009Dokumen203 halamanThe Journal For Baptist Theology and Ministry - Spring 2009Chris SchelinBelum ada peringkat
- Charles Upton - Tradition, Orthodoxy and The Interfaith MovementDokumen0 halamanCharles Upton - Tradition, Orthodoxy and The Interfaith MovementChris SchelinBelum ada peringkat
- Stratford Caldecott - Christian and Hindu Non-Dualism PDFDokumen24 halamanStratford Caldecott - Christian and Hindu Non-Dualism PDFChris SchelinBelum ada peringkat
- The Acts of John as a Gnostic text analyzedDokumen7 halamanThe Acts of John as a Gnostic text analyzedChris SchelinBelum ada peringkat
- Carbon Star Observing Club: The List of Stars No. Name Cat. #: R.A. Dec. Mag. Period ClassDokumen6 halamanCarbon Star Observing Club: The List of Stars No. Name Cat. #: R.A. Dec. Mag. Period ClassChris SchelinBelum ada peringkat
- On Our Way - Christian Practices For Living A Whole LifeDokumen80 halamanOn Our Way - Christian Practices For Living A Whole LifeChris SchelinBelum ada peringkat
- Make Your Own Solar FilterDokumen2 halamanMake Your Own Solar FilterChris SchelinBelum ada peringkat
- Stratford Caldecott - Christian and Hindu Non-Dualism PDFDokumen24 halamanStratford Caldecott - Christian and Hindu Non-Dualism PDFChris SchelinBelum ada peringkat
- Make Your Own Solar FilterDokumen2 halamanMake Your Own Solar FilterChris SchelinBelum ada peringkat
- The Text of Galatians and Its HistoryDokumen384 halamanThe Text of Galatians and Its HistoryChris SchelinBelum ada peringkat
- Is the Soul a Form? Plato's Argument in Phaedo 104-105Dokumen10 halamanIs the Soul a Form? Plato's Argument in Phaedo 104-105Chris SchelinBelum ada peringkat
- Huston Smith - The Universal Grammar of ReligionDokumen11 halamanHuston Smith - The Universal Grammar of ReligionChris SchelinBelum ada peringkat
- Francis Tiso - Evagrius of Pontus and Buddhist AbhidharmaDokumen32 halamanFrancis Tiso - Evagrius of Pontus and Buddhist AbhidharmaChris Schelin100% (1)
- IBTS Writing Style GuideDokumen8 halamanIBTS Writing Style GuideChris SchelinBelum ada peringkat
- Archaeology of NazarethDokumen13 halamanArchaeology of NazarethChris Schelin0% (1)
- Jewish Messiahs, The Pauline Christ, and The Gentile QuestionDokumen18 halamanJewish Messiahs, The Pauline Christ, and The Gentile QuestionChris Schelin100% (1)
- Brian Schultz - Jesus As Archelaus in Parable of PoundsDokumen24 halamanBrian Schultz - Jesus As Archelaus in Parable of PoundsChris SchelinBelum ada peringkat
- Why Christianity Works: An Emotions-Focused Phenomenological AccountDokumen15 halamanWhy Christianity Works: An Emotions-Focused Phenomenological AccountChris SchelinBelum ada peringkat
- David Paul Boaz - Buddhist View of Nature of MindDokumen11 halamanDavid Paul Boaz - Buddhist View of Nature of MindChris SchelinBelum ada peringkat
- Jesus, John, and The Essenes - Robert FeatherDokumen12 halamanJesus, John, and The Essenes - Robert FeatherChris Schelin100% (2)
- Lena Einhorn - Jesus and The Egyptian ProphetDokumen40 halamanLena Einhorn - Jesus and The Egyptian ProphetChris SchelinBelum ada peringkat
- Creative Bible Study Methods For Youth LeadersDokumen60 halamanCreative Bible Study Methods For Youth LeadersChris SchelinBelum ada peringkat
- Ascent To Heaven in Islamic and Jewish Mysticism Excerpt)Dokumen26 halamanAscent To Heaven in Islamic and Jewish Mysticism Excerpt)Chris Schelin100% (1)
- Story SticksDokumen9 halamanStory SticksChris SchelinBelum ada peringkat
- Chris Schelin - in A Congregational Way (JEBS Version)Dokumen16 halamanChris Schelin - in A Congregational Way (JEBS Version)Chris SchelinBelum ada peringkat
- Capnography: Dr. Jacqueline D'Mello Dr. Manju ButaniDokumen10 halamanCapnography: Dr. Jacqueline D'Mello Dr. Manju ButaniMarco Morante VegaBelum ada peringkat
- CompilationDokumen117 halamanCompilationChristian james PazBelum ada peringkat
- Basic Life Support Techniques and ProceduresDokumen7 halamanBasic Life Support Techniques and ProceduresNay ThureinBelum ada peringkat
- Fabfivemodule 2 Envianalysis 1Dokumen14 halamanFabfivemodule 2 Envianalysis 1api-630131676Belum ada peringkat
- Basic Life Support StepsDokumen16 halamanBasic Life Support StepsHend SuryaBelum ada peringkat
- NRP 8 Edition in Canada: A Review of New Recommendations and Their RationaleDokumen32 halamanNRP 8 Edition in Canada: A Review of New Recommendations and Their RationaleRavikiran Suryanarayanamurthy100% (1)
- Pra & Intra Hospital Cardiac Arrest Management-MAHESA Agustus 2021Dokumen65 halamanPra & Intra Hospital Cardiac Arrest Management-MAHESA Agustus 2021Menggy 31Belum ada peringkat
- Introduction - MIDokumen10 halamanIntroduction - MIkhimiiiBelum ada peringkat
- Fire Warden/Fire Marshal Training: Course DescriptionDokumen22 halamanFire Warden/Fire Marshal Training: Course DescriptionCaroline FrostBelum ada peringkat
- Understanding Basic Life Support (BHDDokumen29 halamanUnderstanding Basic Life Support (BHDFadhilah MuthiBelum ada peringkat
- Sepsis 2021 International Guidelines: Mohd Saif KhanDokumen45 halamanSepsis 2021 International Guidelines: Mohd Saif KhanRully ZenBelum ada peringkat
- Sarah DahlDokumen14 halamanSarah DahlFOX 11 NewsBelum ada peringkat
- Suplente Septiembre Lengua Extranjera (Inglés) Examen ADokumen1 halamanSuplente Septiembre Lengua Extranjera (Inglés) Examen AAnonymous zqdKPKoXBelum ada peringkat
- Pseudo-PEA Diagnosis and ManagementDokumen5 halamanPseudo-PEA Diagnosis and Managementmaria Luisa VillaseñorBelum ada peringkat
- Lazarus PhenomenonDokumen6 halamanLazarus PhenomenonWanjaWx3Belum ada peringkat
- CPR Logo - Google SearchDokumen1 halamanCPR Logo - Google SearchRola MohammadBelum ada peringkat
- Victorian Multicultural Commission Summer 2009Dokumen41 halamanVictorian Multicultural Commission Summer 2009Slovenian Webclassroom Topic Resources100% (37)
- Guideline Luka Bakar PDFDokumen50 halamanGuideline Luka Bakar PDFHendry DimasBelum ada peringkat
- P.e12 Lesson Safety ProtocolDokumen23 halamanP.e12 Lesson Safety ProtocolArcLosephBelum ada peringkat
- Intro To First Aid and Basic Life SupportDokumen31 halamanIntro To First Aid and Basic Life SupportLance BaraquielBelum ada peringkat
- BleedingDokumen3 halamanBleedingNor FarehaBelum ada peringkat
- Cmas Oxygen Administration Training ProgrammeDokumen4 halamanCmas Oxygen Administration Training ProgrammeHakim GhilaciBelum ada peringkat
- Basic Life Support (BLS) in AdultsDokumen13 halamanBasic Life Support (BLS) in AdultsElena ChitoiuBelum ada peringkat