Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Credit Card Response Rates and ProfitsDokumen6 halamanCredit Card Response Rates and ProfitskkiiiddBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Common Law Distress On Third PartiesDokumen7 halamanCommon Law Distress On Third Partiesnorris1234Belum ada peringkat
- Toa Consolidated Sample QuestionsDokumen60 halamanToa Consolidated Sample QuestionsBabi Dimaano NavarezBelum ada peringkat
- ICSB Hand BookDokumen39 halamanICSB Hand BookSubarna Saha100% (1)
- Practice Quiz - Review of Working CapitalDokumen9 halamanPractice Quiz - Review of Working Capitalcharisse nuevaBelum ada peringkat
- Statistics 2011 Hiv Surveillance Report Vol 23Dokumen84 halamanStatistics 2011 Hiv Surveillance Report Vol 23api-250472362Belum ada peringkat
- Risk HIV Among Black AA GayDokumen2 halamanRisk HIV Among Black AA GayDavidEppsBelum ada peringkat
- Aetcenews 9Dokumen5 halamanAetcenews 9api-250472362Belum ada peringkat
- Risk TransgenderDokumen2 halamanRisk Transgenderapi-250472362Belum ada peringkat
- Risk WomenDokumen2 halamanRisk Womenapi-250472362Belum ada peringkat
- Paswha Newsletter - November 2011Dokumen4 halamanPaswha Newsletter - November 2011api-250472362Belum ada peringkat
- Ipv and Hiv in WomenDokumen8 halamanIpv and Hiv in Womenapi-250472362Belum ada peringkat
- Risk Hiv AfricanamericansDokumen2 halamanRisk Hiv Africanamericansapi-250472362Belum ada peringkat
- Risk Youth Fact Sheet FinalDokumen2 halamanRisk Youth Fact Sheet Finalapi-250472362Belum ada peringkat
- Aidsvu SoutheastDokumen28 halamanAidsvu Southeastapi-250472362Belum ada peringkat
- Paswha Newsletter - World Aids Day 2013 EditionDokumen7 halamanPaswha Newsletter - World Aids Day 2013 Editionapi-250472362Belum ada peringkat
- Statistics Basics FactsheetDokumen2 halamanStatistics Basics Factsheetapi-250472362Belum ada peringkat
- Paswha Newsletter - First Quarter 2013Dokumen4 halamanPaswha Newsletter - First Quarter 2013api-250472362Belum ada peringkat
- Paswha Newsletter - Second Quarter 2013Dokumen4 halamanPaswha Newsletter - Second Quarter 2013api-250472362Belum ada peringkat
- Paswha Newsletter - March 2012Dokumen4 halamanPaswha Newsletter - March 2012api-250472362Belum ada peringkat
- Paswha Newsletter-April May 2012Dokumen5 halamanPaswha Newsletter-April May 2012api-250472362Belum ada peringkat
- Paswha Newsletter - First Quarter 2014 EditionDokumen7 halamanPaswha Newsletter - First Quarter 2014 Editionapi-250472362Belum ada peringkat
- Paswha Newsletter - 4th Quarter 2012Dokumen5 halamanPaswha Newsletter - 4th Quarter 2012api-250472362Belum ada peringkat
- 8535 Assessing The Impact of The Affordable Care Act On Health Insurance CoverageDokumen15 halaman8535 Assessing The Impact of The Affordable Care Act On Health Insurance Coverageapi-250472362Belum ada peringkat
- QGCT 37Dokumen40 halamanQGCT 37api-250472362Belum ada peringkat
- 03 Cehivaidsconf 14 Flier 2Dokumen4 halaman03 Cehivaidsconf 14 Flier 2api-250472362Belum ada peringkat
- Kapt 37Dokumen14 halamanKapt 37api-250472362Belum ada peringkat
- Health Care Reform and People Living With HivDokumen4 halamanHealth Care Reform and People Living With Hivapi-250472362Belum ada peringkat
- Sma11 4662Dokumen8 halamanSma11 4662api-250472362Belum ada peringkat
- PT. Unilever Indonesia TBK.: Head OfficeDokumen1 halamanPT. Unilever Indonesia TBK.: Head OfficeLinaBelum ada peringkat
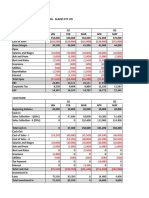
- CMA Case Study Blades PTY LTDDokumen6 halamanCMA Case Study Blades PTY LTDMuhamad ArdiansyahBelum ada peringkat
- FBL Annual Report 2019Dokumen130 halamanFBL Annual Report 2019Fuaad DodooBelum ada peringkat
- TaxDokumen18 halamanTaxPatrickBeronaBelum ada peringkat
- Chapter-Iii Company Profile: Motilal Oswal Financial Services Ltd. (BSE, NIFTY, NASDAQ, Dow Jones, Hang Seng)Dokumen8 halamanChapter-Iii Company Profile: Motilal Oswal Financial Services Ltd. (BSE, NIFTY, NASDAQ, Dow Jones, Hang Seng)MubeenBelum ada peringkat
- 03 BIWS Equity Value Enterprise ValueDokumen6 halaman03 BIWS Equity Value Enterprise ValuecarminatBelum ada peringkat
- Federal ReserveDokumen21 halamanFederal ReserveMsKhan0078Belum ada peringkat
- Jacob Investigates Bretton FraudDokumen2 halamanJacob Investigates Bretton FraudMilcah De GuzmanBelum ada peringkat
- Company Report - Venus Remedies LTDDokumen36 halamanCompany Report - Venus Remedies LTDseema1707Belum ada peringkat
- PFRS 16 Lease Accounting GuideDokumen2 halamanPFRS 16 Lease Accounting GuideQueen ValleBelum ada peringkat
- Understanding Credit Agreement Basics: Deals & FacilitiesDokumen36 halamanUnderstanding Credit Agreement Basics: Deals & FacilitiesJonathan RandallBelum ada peringkat
- Book Review The TCS Story ... and BeyondDokumen4 halamanBook Review The TCS Story ... and BeyondIshanBelum ada peringkat
- IDirect Zomato IPOReviewDokumen13 halamanIDirect Zomato IPOReviewSnehashree SahooBelum ada peringkat
- MAS Annual Report 2010 - 2011Dokumen119 halamanMAS Annual Report 2010 - 2011Ayako S. WatanabeBelum ada peringkat
- Responsibility Accounting and Profitability RatiosDokumen13 halamanResponsibility Accounting and Profitability RatiosKhrystal AbrioBelum ada peringkat
- Fundamentals of Corporate Finance, 2/e: Robert Parrino, Ph.D. David S. Kidwell, Ph.D. Thomas W. Bates, PH.DDokumen50 halamanFundamentals of Corporate Finance, 2/e: Robert Parrino, Ph.D. David S. Kidwell, Ph.D. Thomas W. Bates, PH.DThành NguyễnBelum ada peringkat
- CVP - Quiz 1Dokumen7 halamanCVP - Quiz 1Jane ValenciaBelum ada peringkat
- Coforge LimitedDokumen215 halamanCoforge LimitedJaydev JaydevBelum ada peringkat
- Quant Checklist 463 by Aashish Arora For Bank Exams 2024Dokumen102 halamanQuant Checklist 463 by Aashish Arora For Bank Exams 2024sharpleakeyBelum ada peringkat
- CVPA ANALYSIS AND BEP CALCULATIONSDokumen38 halamanCVPA ANALYSIS AND BEP CALCULATIONSLouie De La TorreBelum ada peringkat
- A2 - AllahabadDokumen2 halamanA2 - AllahabadVbs ReddyBelum ada peringkat
- MilmaDokumen50 halamanMilmaPhilip G Geoji50% (2)
- Ali Mousa and Sons ContractingDokumen1 halamanAli Mousa and Sons ContractingMohsin aliBelum ada peringkat
- Shamik Bhose September Crude Oil ReportDokumen8 halamanShamik Bhose September Crude Oil ReportshamikbhoseBelum ada peringkat
- Cooperative ManualDokumen35 halamanCooperative ManualPratik MogheBelum ada peringkat