Anda mungkin juga menyukai
- Pituitary Tumors: A Clinical CasebookDari EverandPituitary Tumors: A Clinical CasebookLisa B. NachtigallBelum ada peringkat
- Conservative Management of Placenta Accreta in A Multiparous WomanDokumen10 halamanConservative Management of Placenta Accreta in A Multiparous WomanRobel Mae Lagos MontañoBelum ada peringkat
- Placenta Percreta Dan Ligasi Arteri Internal IlliakaDokumen4 halamanPlacenta Percreta Dan Ligasi Arteri Internal IlliakaNyoman TapayanaBelum ada peringkat
- A Cornual Ectopic Pregnancy Case: Diagnosis, Etiology and Its ManagementDokumen5 halamanA Cornual Ectopic Pregnancy Case: Diagnosis, Etiology and Its ManagementparkfishyBelum ada peringkat
- Gynecology and Minimally Invasive Therapy: Shahul Hameed Mohamed Siraj, Bernard Su Min ChernDokumen3 halamanGynecology and Minimally Invasive Therapy: Shahul Hameed Mohamed Siraj, Bernard Su Min ChernIrvin MarcelBelum ada peringkat
- Uterine AtonyDokumen4 halamanUterine AtonyJohn Cenas100% (1)
- Adenomyosis Excision Followed by Successful Live Birth After Three Consecutive IVFDokumen5 halamanAdenomyosis Excision Followed by Successful Live Birth After Three Consecutive IVFPyuzz RemakeBelum ada peringkat
- AkretaDokumen7 halamanAkretaInna SeraLaratBelum ada peringkat
- Anesthetic implications of uterine rupture in a primigravid patientDokumen4 halamanAnesthetic implications of uterine rupture in a primigravid patientYahia AhmadBelum ada peringkat
- A Rare Case of Morbidly Adherent Placenta in A Young - 2024 - International JouDokumen4 halamanA Rare Case of Morbidly Adherent Placenta in A Young - 2024 - International JouRonald QuezadaBelum ada peringkat
- RM 08008Dokumen6 halamanRM 08008Manoj ChoudharyBelum ada peringkat
- Early Pregnancy Problems: Presented byDokumen28 halamanEarly Pregnancy Problems: Presented byMalk OmryBelum ada peringkat
- Ojog 2013020415273326Dokumen6 halamanOjog 2013020415273326Achmad Safi'iBelum ada peringkat
- Cesarean Scar Ectopic Pregnancy Case ReportDokumen6 halamanCesarean Scar Ectopic Pregnancy Case ReportMominah MayamBelum ada peringkat
- Cesarean Scar Pregnancies and Their ManagementDokumen7 halamanCesarean Scar Pregnancies and Their ManagementClinton SitanggangBelum ada peringkat
- New Options for Managing Adherent PlacentaDokumen6 halamanNew Options for Managing Adherent PlacentaAngelique Ramos PascuaBelum ada peringkat
- Managment of Scar PregnancyDokumen43 halamanManagment of Scar Pregnancyvacha sardarBelum ada peringkat
- Minakshi S. Neglected Puerperal Inversion of The Uterus Ignorance Makes Acute A Chronic FormDokumen4 halamanMinakshi S. Neglected Puerperal Inversion of The Uterus Ignorance Makes Acute A Chronic FormJulius Albert SBelum ada peringkat
- An Interesting Case of Intramyometrial Pregnancy: Rare DiseaseDokumen5 halamanAn Interesting Case of Intramyometrial Pregnancy: Rare DiseaseDinorah MarcelaBelum ada peringkat
- Yan 2007Dokumen3 halamanYan 2007Agustin LindaBelum ada peringkat
- JurnalDokumen4 halamanJurnalMigumi YoshugaraBelum ada peringkat
- CCD - Ectopic Pregnancy HafyzDokumen29 halamanCCD - Ectopic Pregnancy HafyzHanif GandohBelum ada peringkat
- Ectopic Pregnancy: Causes, Symptoms and Treatment OptionsDokumen12 halamanEctopic Pregnancy: Causes, Symptoms and Treatment OptionsAnni BarbaBelum ada peringkat
- 10 1016@j Ijscr 2020 01 020Dokumen4 halaman10 1016@j Ijscr 2020 01 020ari naBelum ada peringkat
- Practice Bulletin: Medical Management of Ectopic PregnancyDokumen7 halamanPractice Bulletin: Medical Management of Ectopic PregnancyChangBelum ada peringkat
- Placenta Previa 1Dokumen2 halamanPlacenta Previa 1Gunther MirandaBelum ada peringkat
- Laparoscopy During PregnancyDokumen6 halamanLaparoscopy During PregnancyTrần Ngọc TúBelum ada peringkat
- Blighted Ovum: A Case ReportDokumen2 halamanBlighted Ovum: A Case Reportakhmad ikhwanBelum ada peringkat
- Ectopic Pregnancy Diagnosis and TreatmentDokumen39 halamanEctopic Pregnancy Diagnosis and TreatmentFecky Fihayatul IchsanBelum ada peringkat
- Endometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDokumen4 halamanEndometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDikie MustofadijayaBelum ada peringkat
- Clinical Study: Nitroglycerin For Management of Retained Placenta: A Multicenter StudyDokumen7 halamanClinical Study: Nitroglycerin For Management of Retained Placenta: A Multicenter StudyTri Anna FitrianiBelum ada peringkat
- Effectiveness of Per Rectal Misoprostol Versus Intramuscular Oxytocin For Prevention of Primary Postpartum HaemorrhageDokumen5 halamanEffectiveness of Per Rectal Misoprostol Versus Intramuscular Oxytocin For Prevention of Primary Postpartum HaemorrhageFuad HasanBelum ada peringkat
- Artículo Nefro 2Dokumen6 halamanArtículo Nefro 2Stephani RobinsonBelum ada peringkat
- An Alternative To Hysterectomy: Manchester RepairDokumen0 halamanAn Alternative To Hysterectomy: Manchester RepairDwi WicaksonoBelum ada peringkat
- Hemorragia y EmbrazoDokumen6 halamanHemorragia y Embrazoana catalinaBelum ada peringkat
- Conservative Management of Ectopic Pregnancy: A Provincial Hospital Case Series of Medically Managed Ectopic PregnanciesDokumen5 halamanConservative Management of Ectopic Pregnancy: A Provincial Hospital Case Series of Medically Managed Ectopic PregnanciesSandy JusiBelum ada peringkat
- Imafuku 2019Dokumen5 halamanImafuku 2019Rizki FebriyaniBelum ada peringkat
- Hetero TopicDokumen3 halamanHetero TopicDONNYBelum ada peringkat
- tmp7DB6 TMPDokumen78 halamantmp7DB6 TMPFrontiersBelum ada peringkat
- Clinical Presentation of Ectopic Pregnancy Turned Out to Be Ectopic PregnancyDokumen33 halamanClinical Presentation of Ectopic Pregnancy Turned Out to Be Ectopic PregnancyRosiBelum ada peringkat
- Willmott Et Al-2008-BJOG An International Journal of Obstetrics & GynaecologyDokumen3 halamanWillmott Et Al-2008-BJOG An International Journal of Obstetrics & GynaecologyganangahimsaBelum ada peringkat
- Best modality for diagnosing ectopic pregnancyDokumen31 halamanBest modality for diagnosing ectopic pregnancyantonio91uBelum ada peringkat
- Acute Abdomen in PregnancyDokumen6 halamanAcute Abdomen in PregnancydkasisBelum ada peringkat
- Managing Placenta Accreta: Medical vs Surgical OptionsDokumen9 halamanManaging Placenta Accreta: Medical vs Surgical OptionsAslesa Wangpathi PagehgiriBelum ada peringkat
- Mifepristone and Misoprostol For Early Pregnancy Failure: A Cohort AnalysisDokumen6 halamanMifepristone and Misoprostol For Early Pregnancy Failure: A Cohort AnalysisBobby SetiawanBelum ada peringkat
- Embarazo EctópicoDokumen7 halamanEmbarazo EctópicomariBelum ada peringkat
- Nama: Zaimah Shalsabilla Kelas: Alpha NIM: 04011181520071Dokumen11 halamanNama: Zaimah Shalsabilla Kelas: Alpha NIM: 04011181520071shalsaBelum ada peringkat
- W 3 e WDDokumen6 halamanW 3 e WDsupaidi97Belum ada peringkat
- UC Irvine: Clinical Practice and Cases in Emergency MedicineDokumen6 halamanUC Irvine: Clinical Practice and Cases in Emergency MedicinePatrick NunsioBelum ada peringkat
- Journal Gyn KETDokumen8 halamanJournal Gyn KETImaylani S. SitanggangBelum ada peringkat
- Uterine Inversion: A Life-Threatening Obstetric Emergency: Dawn R. Hostetler, MD, and Michael Bosworth, DODokumen4 halamanUterine Inversion: A Life-Threatening Obstetric Emergency: Dawn R. Hostetler, MD, and Michael Bosworth, DOAndi Farras WatyBelum ada peringkat
- 1 s2.0 S2211419X13000578 MainDokumen4 halaman1 s2.0 S2211419X13000578 Mainindra040293Belum ada peringkat
- Csii-Pregnancy in Patients With Mechanical Prosthetic ValvesDokumen6 halamanCsii-Pregnancy in Patients With Mechanical Prosthetic Valvesapi-205989841Belum ada peringkat
- Hioerplasia Mamaria GestacionalDokumen9 halamanHioerplasia Mamaria GestacionalOctavio LeyvaBelum ada peringkat
- Aderoba 2016Dokumen8 halamanAderoba 2016DONNYBelum ada peringkat
- Uog 14728Dokumen25 halamanUog 14728Stanley PhanBelum ada peringkat
- Women's Health Case: Methotrexate vs Laparoscopic SalpingostomyDokumen9 halamanWomen's Health Case: Methotrexate vs Laparoscopic SalpingostomyWong Chui YeeBelum ada peringkat
- tmpC705 TMPDokumen3 halamantmpC705 TMPFrontiersBelum ada peringkat
- tmpB9EA TMPDokumen3 halamantmpB9EA TMPFrontiersBelum ada peringkat
- Tugas English Lesson 12-14 FIXDokumen1 halamanTugas English Lesson 12-14 FIXDeddy AngBelum ada peringkat
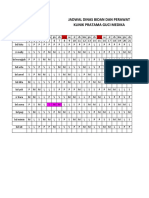
- Jadwal Dinas Bidan Dan Perawat Klinik Pratama Guci MedikaDokumen5 halamanJadwal Dinas Bidan Dan Perawat Klinik Pratama Guci MedikaDeddy AngBelum ada peringkat
- AdvBiomedRes2120-8335885 230918Dokumen4 halamanAdvBiomedRes2120-8335885 230918Deddy AngBelum ada peringkat
- Acute Necrotizing Ulcerative GingivitisDokumen9 halamanAcute Necrotizing Ulcerative GingivitisDeddy AngBelum ada peringkat
- Daftar PustakaDokumen3 halamanDaftar PustakaDeddy AngBelum ada peringkat
- Presentation1 DaraDokumen20 halamanPresentation1 DaraDeddy AngBelum ada peringkat
- LTE EPC Technical OverviewDokumen320 halamanLTE EPC Technical OverviewCristian GuleiBelum ada peringkat
- 3GPP TS 36.306Dokumen131 halaman3GPP TS 36.306Tuan DaoBelum ada peringkat
- Theoretical and Actual CombustionDokumen14 halamanTheoretical and Actual CombustionErma Sulistyo R100% (1)
- Project Binder 2Dokumen23 halamanProject Binder 2Singh DhirendraBelum ada peringkat
- TIA Selection Tool: Release Notes V2022.05Dokumen10 halamanTIA Selection Tool: Release Notes V2022.05Patil Amol PandurangBelum ada peringkat
- Datasheet PDFDokumen6 halamanDatasheet PDFAhmed ElShoraBelum ada peringkat
- Flowing Gas Material BalanceDokumen4 halamanFlowing Gas Material BalanceVladimir PriescuBelum ada peringkat
- Sradham ChecklistDokumen9 halamanSradham ChecklistpswaminathanBelum ada peringkat
- Religion in Space Science FictionDokumen23 halamanReligion in Space Science FictionjasonbattBelum ada peringkat
- Emerson EPC48150 1800 FA1EPC48300 3200 FA1 V PDFDokumen26 halamanEmerson EPC48150 1800 FA1EPC48300 3200 FA1 V PDFRicardo Andrés Soto Salinas RassBelum ada peringkat
- A Fossil Hunting Guide To The Tertiary Formations of Qatar, Middle-EastDokumen82 halamanA Fossil Hunting Guide To The Tertiary Formations of Qatar, Middle-EastJacques LeBlanc100% (18)
- Survey Report on Status of Chemical and Microbiological Laboratories in NepalDokumen38 halamanSurvey Report on Status of Chemical and Microbiological Laboratories in NepalGautam0% (1)
- Reflection 2: WHAT DOES It Mean To Be A Pacific Islander Today and in The Future To Me?Dokumen5 halamanReflection 2: WHAT DOES It Mean To Be A Pacific Islander Today and in The Future To Me?Trishika NamrataBelum ada peringkat
- 1989 GMC Light Duty Truck Fuel and Emissions Including Driveability PDFDokumen274 halaman1989 GMC Light Duty Truck Fuel and Emissions Including Driveability PDFRobert Klitzing100% (1)
- Tds G. Beslux Komplex Alfa II (25.10.19)Dokumen3 halamanTds G. Beslux Komplex Alfa II (25.10.19)Iulian BarbuBelum ada peringkat
- 7890 Parts-Guide APDokumen4 halaman7890 Parts-Guide APZia HaqBelum ada peringkat
- Fundermax Exterior Technic 2011gb WebDokumen88 halamanFundermax Exterior Technic 2011gb WebarchpavlovicBelum ada peringkat
- g4 - Stress Analysis of Operating Gas Pipeline Installed by HorizontalDokumen144 halamang4 - Stress Analysis of Operating Gas Pipeline Installed by HorizontalDevin DickenBelum ada peringkat
- Reflective Essay 4Dokumen1 halamanReflective Essay 4Thirdy AngelesBelum ada peringkat
- 1.2 - Sewing Machine and Special AttachmentsDokumen3 halaman1.2 - Sewing Machine and Special Attachmentsmaya_muth0% (1)
- Are Hypomineralized Primary Molars and Canines Associated With Molar-Incisor HypomineralizationDokumen5 halamanAre Hypomineralized Primary Molars and Canines Associated With Molar-Incisor HypomineralizationDr Chevyndra100% (1)
- Daftar Spesifikasi Teknis Pembangunan Gedung Kantor BPN BojonegoroDokumen6 halamanDaftar Spesifikasi Teknis Pembangunan Gedung Kantor BPN BojonegoroIrwin DarmansyahBelum ada peringkat
- Telco XPOL MIMO Industrial Class Solid Dish AntennaDokumen4 halamanTelco XPOL MIMO Industrial Class Solid Dish AntennaOmar PerezBelum ada peringkat
- WOOD Investor Presentation 3Q21Dokumen65 halamanWOOD Investor Presentation 3Q21Koko HadiwanaBelum ada peringkat
- Organizing Small Items with Glass Bottle OrganizersDokumen70 halamanOrganizing Small Items with Glass Bottle OrganizersDy SaiBelum ada peringkat
- A Compilation of Thread Size InformationDokumen9 halamanA Compilation of Thread Size Informationdim059100% (2)
- CP 343-1Dokumen23 halamanCP 343-1Yahya AdamBelum ada peringkat
- BCP-8000 User's ManualDokumen36 halamanBCP-8000 User's ManualAsad PatelBelum ada peringkat
- Baseline Program Rev 3A Presentation 25 July 2020Dokumen24 halamanBaseline Program Rev 3A Presentation 25 July 2020Shakti Sourava RautrayaBelum ada peringkat
- ML AiDokumen2 halamanML AiSUYASH SHARTHIBelum ada peringkat