Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Compressive Strength Beam DesignDokumen70 halamanCompressive Strength Beam DesignDjuned0% (1)
- 2CG ELTT2 KS TitanMagazine Anazelle-Shan PromoDokumen12 halaman2CG ELTT2 KS TitanMagazine Anazelle-Shan PromoJohn SmithBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- ASME Y14.6-2001 (R2007), Screw Thread RepresentationDokumen27 halamanASME Y14.6-2001 (R2007), Screw Thread RepresentationDerekBelum ada peringkat
- 01-Azeotropic Distillation (IL Chien)Dokumen35 halaman01-Azeotropic Distillation (IL Chien)Shivam Vinoth100% (1)
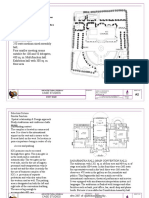
- International Convention Center, BanesworDokumen18 halamanInternational Convention Center, BanesworSreeniketh ChikuBelum ada peringkat
- Asian Construction Dispute Denied ReviewDokumen2 halamanAsian Construction Dispute Denied ReviewJay jogs100% (2)
- Alfa Laval Complete Fittings CatalogDokumen224 halamanAlfa Laval Complete Fittings CatalogGraciele SoaresBelum ada peringkat
- Lake Wood OrdinanceDokumen15 halamanLake Wood OrdinancecwadotorgBelum ada peringkat
- State of Colorado: Second Regular Session Sixty-Seventh General AssemblyDokumen11 halamanState of Colorado: Second Regular Session Sixty-Seventh General AssemblycwadotorgBelum ada peringkat
- LittleTon OrdinanceDokumen20 halamanLittleTon OrdinancecwadotorgBelum ada peringkat
- Amend The Section 0.1 Definition of Home Occupation To ReadDokumen4 halamanAmend The Section 0.1 Definition of Home Occupation To ReadcwadotorgBelum ada peringkat
- Denver City Council MMJ OrdinanceDokumen8 halamanDenver City Council MMJ OrdinancecwadotorgBelum ada peringkat
- BoulderOrd NotesDokumen13 halamanBoulderOrd NotescwadotorgBelum ada peringkat
- City of Cortez Ordinance No. 1135, Series 2010Dokumen3 halamanCity of Cortez Ordinance No. 1135, Series 2010cwadotorgBelum ada peringkat
- Crested Butte OrdDokumen27 halamanCrested Butte OrdcwadotorgBelum ada peringkat
- Ordinance No. 998Dokumen5 halamanOrdinance No. 998cwadotorgBelum ada peringkat
- State of Colorado: Second Regular Session Sixty-Seventh General AssemblyDokumen64 halamanState of Colorado: Second Regular Session Sixty-Seventh General AssemblycwadotorgBelum ada peringkat
- Central City OrdDokumen2 halamanCentral City OrdcwadotorgBelum ada peringkat
- MMR Change of Address BacksideDokumen1 halamanMMR Change of Address BacksidecwadotorgBelum ada peringkat
- Central City AppDokumen8 halamanCentral City AppcwadotorgBelum ada peringkat
- BoulderOrd NotesDokumen13 halamanBoulderOrd NotescwadotorgBelum ada peringkat
- Denver License ApplicationDokumen2 halamanDenver License ApplicationcwadotorgBelum ada peringkat
- Second Regular Session Sixty-Seventh General AssemblyDokumen45 halamanSecond Regular Session Sixty-Seventh General AssemblyCircuit MediaBelum ada peringkat
- Under 18 MMJApplication PackageDokumen5 halamanUnder 18 MMJApplication PackagecwadotorgBelum ada peringkat
- MMR Change of AddressDokumen1 halamanMMR Change of AddresscwadotorgBelum ada peringkat
- Report of Missing or Stolen Medical MarijuanaDokumen1 halamanReport of Missing or Stolen Medical MarijuanacwadotorgBelum ada peringkat
- Multiple Files Are Bound Together in This PDF Package.: Click Here To Download The Latest Version of Adobe ReaderDokumen1 halamanMultiple Files Are Bound Together in This PDF Package.: Click Here To Download The Latest Version of Adobe ReadercwadotorgBelum ada peringkat
- State of Colorado: Second Regular Session Sixty-Seventh General AssemblyDokumen11 halamanState of Colorado: Second Regular Session Sixty-Seventh General AssemblycwadotorgBelum ada peringkat
- Request For Patient InformationDokumen1 halamanRequest For Patient InformationcwadotorgBelum ada peringkat
- Physician CertificationDokumen1 halamanPhysician CertificationcwadotorgBelum ada peringkat
- MMJ Application InstructionsDokumen1 halamanMMJ Application InstructionscwadotorgBelum ada peringkat
- MMJ Registry Application FormDokumen1 halamanMMJ Registry Application FormcwadotorgBelum ada peringkat
- State of Colorado: Second Regular Session Sixty-Seventh General AssemblyDokumen9 halamanState of Colorado: Second Regular Session Sixty-Seventh General AssemblyCircuit MediaBelum ada peringkat
- Law Enforcement Verification ProceduresDokumen3 halamanLaw Enforcement Verification ProcedurescwadotorgBelum ada peringkat
- Petitioning To Add Debilitating Medical ConditionsDokumen1 halamanPetitioning To Add Debilitating Medical ConditionscwadotorgBelum ada peringkat
- Petitioning To Add Debilitating Medical ConditionsDokumen1 halamanPetitioning To Add Debilitating Medical ConditionscwadotorgBelum ada peringkat
- Proposal Semister ProjectDokumen7 halamanProposal Semister ProjectMuket AgmasBelum ada peringkat
- ITS America's 2009 Annual Meeting & Exposition: Preliminary ProgramDokumen36 halamanITS America's 2009 Annual Meeting & Exposition: Preliminary ProgramITS AmericaBelum ada peringkat
- Model:: Powered by CUMMINSDokumen4 halamanModel:: Powered by CUMMINSСергейBelum ada peringkat
- CTS experiments comparisonDokumen2 halamanCTS experiments comparisonmanojkumarBelum ada peringkat
- 2022 Product Catalog WebDokumen100 halaman2022 Product Catalog WebEdinson Reyes ValderramaBelum ada peringkat
- Nature and Effects of ObligationsDokumen5 halamanNature and Effects of ObligationsIan RanilopaBelum ada peringkat
- DrugDokumen2 halamanDrugSaleha YounusBelum ada peringkat
- MSDS Summary: Discover HerbicideDokumen6 halamanMSDS Summary: Discover HerbicideMishra KewalBelum ada peringkat
- Gerhard Budin PublicationsDokumen11 halamanGerhard Budin Publicationshnbc010Belum ada peringkat
- Gps Anti Jammer Gpsdome - Effective Protection Against JammingDokumen2 halamanGps Anti Jammer Gpsdome - Effective Protection Against JammingCarlos VillegasBelum ada peringkat
- Operation Roman Empire Indictment Part 1Dokumen50 halamanOperation Roman Empire Indictment Part 1Southern California Public RadioBelum ada peringkat
- Econometrics Chapter 1 7 2d AgEc 1Dokumen89 halamanEconometrics Chapter 1 7 2d AgEc 1Neway AlemBelum ada peringkat
- The Human Resource Department of GIK InstituteDokumen1 halamanThe Human Resource Department of GIK InstitutexandercageBelum ada peringkat
- WitepsolDokumen21 halamanWitepsolAnastasius HendrianBelum ada peringkat
- Discursive Closure and Discursive Openings in SustainabilityDokumen10 halamanDiscursive Closure and Discursive Openings in SustainabilityRenn MBelum ada peringkat
- CadLink Flyer 369044 937 Rev 00Dokumen2 halamanCadLink Flyer 369044 937 Rev 00ShanaHBelum ada peringkat
- Comparing Time Series Models to Predict Future COVID-19 CasesDokumen31 halamanComparing Time Series Models to Predict Future COVID-19 CasesManoj KumarBelum ada peringkat
- Dissolved Oxygen Primary Prod Activity1Dokumen7 halamanDissolved Oxygen Primary Prod Activity1api-235617848Belum ada peringkat
- Project The Ant Ranch Ponzi Scheme JDDokumen7 halamanProject The Ant Ranch Ponzi Scheme JDmorraz360Belum ada peringkat
- An4856 Stevalisa172v2 2 KW Fully Digital Ac DC Power Supply Dsmps Evaluation Board StmicroelectronicsDokumen74 halamanAn4856 Stevalisa172v2 2 KW Fully Digital Ac DC Power Supply Dsmps Evaluation Board StmicroelectronicsStefano SalaBelum ada peringkat
- Nature of ConversionDokumen18 halamanNature of ConversionKiranBelum ada peringkat
- Software EngineeringDokumen3 halamanSoftware EngineeringImtiyaz BashaBelum ada peringkat
- BAM PPT 2011-09 Investor Day PDFDokumen171 halamanBAM PPT 2011-09 Investor Day PDFRocco HuangBelum ada peringkat