Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Vendor Registration FormDokumen4 halamanVendor Registration FormhiringBelum ada peringkat
- Investigation Data FormDokumen1 halamanInvestigation Data Formnildin danaBelum ada peringkat
- Tec066 6700 PDFDokumen2 halamanTec066 6700 PDFExclusivo VIPBelum ada peringkat
- Bharti Airtel Strategy FinalDokumen39 halamanBharti Airtel Strategy FinalniksforloveuBelum ada peringkat
- Flight Data Recorder Rule ChangeDokumen7 halamanFlight Data Recorder Rule ChangeIgnacio ZupaBelum ada peringkat
- BAMDokumen111 halamanBAMnageswara_mutyalaBelum ada peringkat
- Dependent ClauseDokumen28 halamanDependent ClauseAndi Febryan RamadhaniBelum ada peringkat
- Joomag 2020 06 12 27485398153Dokumen2 halamanJoomag 2020 06 12 27485398153Vincent Deodath Bang'araBelum ada peringkat
- Extraction of Mangiferin From Mangifera Indica L. LeavesDokumen7 halamanExtraction of Mangiferin From Mangifera Indica L. LeavesDaniel BartoloBelum ada peringkat
- 3) Uses and Gratification: 1) The Hypodermic Needle ModelDokumen5 halaman3) Uses and Gratification: 1) The Hypodermic Needle ModelMarikaMcCambridgeBelum ada peringkat
- Present Tenses ExercisesDokumen4 halamanPresent Tenses Exercisesmonkeynotes100% (1)
- Visi RuleDokumen6 halamanVisi RuleBruce HerreraBelum ada peringkat
- PRESENTACIÒN EN POWER POINT Futuro SimpleDokumen5 halamanPRESENTACIÒN EN POWER POINT Futuro SimpleDiego BenítezBelum ada peringkat
- 1KHW001492de Tuning of ETL600 TX RF Filter E5TXDokumen7 halaman1KHW001492de Tuning of ETL600 TX RF Filter E5TXSalvador FayssalBelum ada peringkat
- Communication Skill - Time ManagementDokumen18 halamanCommunication Skill - Time ManagementChấn NguyễnBelum ada peringkat
- Aharonov-Bohm Effect WebDokumen5 halamanAharonov-Bohm Effect Webatactoulis1308Belum ada peringkat
- Subeeka Akbar Advance NutritionDokumen11 halamanSubeeka Akbar Advance NutritionSubeeka AkbarBelum ada peringkat
- Brain Injury Patients Have A Place To Be Themselves: WHY WHYDokumen24 halamanBrain Injury Patients Have A Place To Be Themselves: WHY WHYDonna S. SeayBelum ada peringkat
- Pediatric Fever of Unknown Origin: Educational GapDokumen14 halamanPediatric Fever of Unknown Origin: Educational GapPiegl-Gulácsy VeraBelum ada peringkat
- EC 2012 With SolutionsDokumen50 halamanEC 2012 With Solutionsprabhjot singh1Belum ada peringkat
- The One With The ThumbDokumen4 halamanThe One With The Thumbnoelia20_09Belum ada peringkat
- An Enhanced Radio Network Planning Methodology For GSM-R CommunicationsDokumen4 halamanAn Enhanced Radio Network Planning Methodology For GSM-R CommunicationsNuno CotaBelum ada peringkat
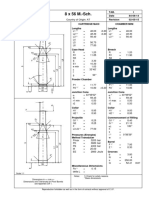
- 8 X 56 M.-SCH.: Country of Origin: ATDokumen1 halaman8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimBelum ada peringkat
- DBM Uv W ChartDokumen2 halamanDBM Uv W ChartEddie FastBelum ada peringkat
- Previews 1633186 PreDokumen11 halamanPreviews 1633186 PreDavid MorenoBelum ada peringkat
- Solutions DPP 2Dokumen3 halamanSolutions DPP 2Tech. VideciousBelum ada peringkat
- 1Dokumen2 halaman1TrầnLanBelum ada peringkat
- EP07 Measuring Coefficient of Viscosity of Castor OilDokumen2 halamanEP07 Measuring Coefficient of Viscosity of Castor OilKw ChanBelum ada peringkat
- MEMORANDUM OF AGREEMENT DraftsDokumen3 halamanMEMORANDUM OF AGREEMENT DraftsRichard Colunga80% (5)
- Kiraan Supply Mesin AutomotifDokumen6 halamanKiraan Supply Mesin Automotifjamali sadatBelum ada peringkat