Anda mungkin juga menyukai
- Analisis Desain Formulir Ringkasan Masuk & Keluar PDFDokumen13 halamanAnalisis Desain Formulir Ringkasan Masuk & Keluar PDFNova Dwi Pawestri II0% (1)
- EmrDokumen8 halamanEmrAnnisa DarmawangsaBelum ada peringkat
- Asesmen Kesiapan Implementasi RME - Handout-1Dokumen36 halamanAsesmen Kesiapan Implementasi RME - Handout-1Bening Ananing100% (1)
- Kode Kombinasi & Kode GandaDokumen15 halamanKode Kombinasi & Kode GandaJuwitahasugianBelum ada peringkat
- Aspek Keamanan BerkasDokumen7 halamanAspek Keamanan BerkassivaBelum ada peringkat
- Soal External Cause 1-8Dokumen7 halamanSoal External Cause 1-8Widiati AfBelum ada peringkat
- KKPMT EndokrinDokumen6 halamanKKPMT EndokrinDyah CitraBelum ada peringkat
- Soal Latihan Tindakan Icd9 CMDokumen3 halamanSoal Latihan Tindakan Icd9 CMArmann100% (1)
- Tugas Praktikum Kodefikasi PenyakitDokumen6 halamanTugas Praktikum Kodefikasi Penyakitdewi candra agustinBelum ada peringkat
- LEMBAR JAWABAN KKPMT 1 - 10 (External Causes (01 November 2021) - (1) - 3Dokumen4 halamanLEMBAR JAWABAN KKPMT 1 - 10 (External Causes (01 November 2021) - (1) - 3Dyah CitraBelum ada peringkat
- Dampak Penumpukan Berkas Rekam Medis Di RuangfilingDokumen12 halamanDampak Penumpukan Berkas Rekam Medis Di RuangfilingKintan IntanBelum ada peringkat
- 2B Dyah Citra Resmi 195055 (KKPMT Sistem Saraf)Dokumen5 halaman2B Dyah Citra Resmi 195055 (KKPMT Sistem Saraf)Dyah CitraBelum ada peringkat
- Rongga Mulut, Kelenjar Saliva Dan Rahang: No Istilah Terminologi Medis Istilah Arti Sumber ReferensiDokumen30 halamanRongga Mulut, Kelenjar Saliva Dan Rahang: No Istilah Terminologi Medis Istilah Arti Sumber ReferensiAlfi Melinda FBelum ada peringkat
- Peranan Kompetensi PMIK Di PuskesmasDokumen101 halamanPeranan Kompetensi PMIK Di Puskesmasahmad 85Belum ada peringkat
- Evaluasi Implementa Si Sistem Electronic Health PDFDokumen14 halamanEvaluasi Implementa Si Sistem Electronic Health PDFSuci RahayuBelum ada peringkat
- Nisa's eye exam diagnosesDokumen4 halamanNisa's eye exam diagnosesNisaadivaBelum ada peringkat
- KODEDokumen14 halamanKODEDeeLha RamadhanaBelum ada peringkat
- MMDS (Medical Morrtality Data System)Dokumen1.241 halamanMMDS (Medical Morrtality Data System)Bhella GuntoroBelum ada peringkat
- Latihan Soal Chapter XVDokumen15 halamanLatihan Soal Chapter XVDEWI WULANDARI KONTJE100% (1)
- Tinjauan Penerapan Sistem Rekam Medis Elektronik Rawat Jalan Di Rumah Sakit Pelabuhan JakartaDokumen5 halamanTinjauan Penerapan Sistem Rekam Medis Elektronik Rawat Jalan Di Rumah Sakit Pelabuhan JakartaAndi GumelarBelum ada peringkat
- Icpc Pembahasan Coding Dengan IcpcDokumen52 halamanIcpc Pembahasan Coding Dengan IcpcMelita RamadhaniBelum ada peringkat
- Kodifikasi Latihan Chapter XVDokumen3 halamanKodifikasi Latihan Chapter XVZidaneBelum ada peringkat
- 07 - Hit Readiness AssessmentDokumen13 halaman07 - Hit Readiness AssessmentAbidi HichemBelum ada peringkat
- BS Rekam Medis Dan KerahasiaanDokumen93 halamanBS Rekam Medis Dan KerahasiaanCeceBelum ada peringkat
- CodingDokumen110 halamanCodingBudi Yunanto100% (1)
- Kode Diagnosis Dan Tindakan Sistem Panca IndraDokumen3 halamanKode Diagnosis Dan Tindakan Sistem Panca IndraNitaNurmalaBelum ada peringkat
- Uswatun Hasanah-195037-2a Rmik (KKPMT)Dokumen4 halamanUswatun Hasanah-195037-2a Rmik (KKPMT)Uswatun HasanahBelum ada peringkat
- KKPMT Cidera Dan KeracunanDokumen4 halamanKKPMT Cidera Dan KeracunanDyah CitraBelum ada peringkat
- Soal Praktik Bab XII KodifikasiDokumen2 halamanSoal Praktik Bab XII KodifikasiBil100% (1)
- Terminologi MedisDokumen17 halamanTerminologi MedisRanie Zt67% (3)
- Form Registrasi Kanker RSDokumen10 halamanForm Registrasi Kanker RSAnonymous 8UVWsABelum ada peringkat
- Form Registrasi Kanker RSDokumen10 halamanForm Registrasi Kanker RSRika WandiBelum ada peringkat
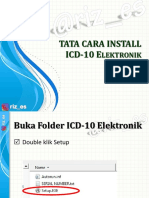
- TATA CARA INSTALL ICD-10 ElektronikDokumen6 halamanTATA CARA INSTALL ICD-10 ElektronikPuskesmas Cijagra BaruBelum ada peringkat
- 3b-195055-Dyah Citra Resmi (KKPMT Kulit)Dokumen3 halaman3b-195055-Dyah Citra Resmi (KKPMT Kulit)Dyah CitraBelum ada peringkat
- PMK 21/2020: Menuju Rekam Medis Elektronik (RME) TerintegrasiDokumen22 halamanPMK 21/2020: Menuju Rekam Medis Elektronik (RME) TerintegrasiDony KristianBelum ada peringkat
- Latihan Soal Koding PerinatalDokumen9 halamanLatihan Soal Koding PerinatalikaBelum ada peringkat
- ICECI Classification for External Causes of InjuryDokumen21 halamanICECI Classification for External Causes of InjuryMona MeidyaBelum ada peringkat
- Pedoman Retensi Rekam Medis (Dr. Rano Indradi, M.kes)Dokumen20 halamanPedoman Retensi Rekam Medis (Dr. Rano Indradi, M.kes)febi novrizalBelum ada peringkat
- Kode Pintar ICD 9 CMDokumen1 halamanKode Pintar ICD 9 CMjack poetraBelum ada peringkat
- Kelmpok 3 Jawaban Soal 1 SD 10Dokumen50 halamanKelmpok 3 Jawaban Soal 1 SD 10tri lestariBelum ada peringkat
- Nama: Dyah Citra Resmi Nim: 195055 Kelas: 3B RMIKDokumen3 halamanNama: Dyah Citra Resmi Nim: 195055 Kelas: 3B RMIKDyah CitraBelum ada peringkat
- Penerapan Man Resiko Unit Filing Rsud DR MoewardiDokumen8 halamanPenerapan Man Resiko Unit Filing Rsud DR Moewardibina makmurBelum ada peringkat
- KODINGDokumen5 halamanKODINGDesy RusianaBelum ada peringkat
- Analisis Kuantitatif Kelengkapan Dokumen Rekam Medis Pasien RawatDokumen10 halamanAnalisis Kuantitatif Kelengkapan Dokumen Rekam Medis Pasien RawatLahasang JieBelum ada peringkat
- Dyah Citra Resmi medical diagnosesDokumen4 halamanDyah Citra Resmi medical diagnosesDyah CitraBelum ada peringkat
- Paradigma Baru Pengelolaan Keuangan Rumah SakitDokumen17 halamanParadigma Baru Pengelolaan Keuangan Rumah SakitQaisha ArbeyBelum ada peringkat
- Paper Consultation & ConsolidationDokumen11 halamanPaper Consultation & ConsolidationSindy RosdianasBelum ada peringkat
- Daftar KODE ICD-9 Bedah Saraf (Kode)Dokumen5 halamanDaftar KODE ICD-9 Bedah Saraf (Kode)ema100% (3)
- Kode IcdDokumen34 halamanKode IcdAriefz Will100% (1)
- MIRM ELEMEN PENILAIANDokumen25 halamanMIRM ELEMEN PENILAIANICHA100% (5)
- Kel7 Unit3 BHS InggrisDokumen8 halamanKel7 Unit3 BHS Inggrisrafiqa gustinaBelum ada peringkat
- Tugas Coding Aulia Zajila Rmik 4aDokumen2 halamanTugas Coding Aulia Zajila Rmik 4aAulia ZajilaBelum ada peringkat
- Morbiditas Rawat Inap Dan Jalan RSIA Husada BundaDokumen4 halamanMorbiditas Rawat Inap Dan Jalan RSIA Husada BundameldonosepoetroBelum ada peringkat
- Soal Ukom Rekam Medis 50 Soal Level 3Dokumen14 halamanSoal Ukom Rekam Medis 50 Soal Level 3ayuciBelum ada peringkat
- Analisis Pelaksanaan Retensi Dan Penyimpanan Dokumen Rekam Medis Inaktif Filing Rawat Jalan Di Rumah Sakit Bhayangkara Semarang Tahun 2016Dokumen11 halamanAnalisis Pelaksanaan Retensi Dan Penyimpanan Dokumen Rekam Medis Inaktif Filing Rawat Jalan Di Rumah Sakit Bhayangkara Semarang Tahun 2016Haris ArisBelum ada peringkat
- Kode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2018Dokumen13 halamanKode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2018EkaChandraBelum ada peringkat
- Kode Pintar Icd 9 CMDokumen4 halamanKode Pintar Icd 9 CMarisBelum ada peringkat
- The Eight Components of Integrated Service ManagementDokumen3 halamanThe Eight Components of Integrated Service ManagementRohan Singh100% (1)
- Data Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareDari EverandData Makes the Difference: The Smart Nurse's Handbook for Using Data to Improve CareBelum ada peringkat
- Meeting Health Information Needs Outside Of Healthcare: Opportunities and ChallengesDari EverandMeeting Health Information Needs Outside Of Healthcare: Opportunities and ChallengesBelum ada peringkat
- Lesson PlanDokumen2 halamanLesson Planapi-283246674Belum ada peringkat
- Return To Work FormDokumen1 halamanReturn To Work Formair2212Belum ada peringkat
- 1535 5714 1 PBDokumen5 halaman1535 5714 1 PBSuriyusufipratiwiBelum ada peringkat
- Anti Aging Health Benefits of YogaDokumen5 halamanAnti Aging Health Benefits of Yogasourav.surBelum ada peringkat
- Chinese - Zhong Yi Zhen Duan Xue - Diagnostics of TCMDokumen578 halamanChinese - Zhong Yi Zhen Duan Xue - Diagnostics of TCMalbertomtch94% (33)
- Nursing Information SystemDokumen1 halamanNursing Information SystemDesi Ratna YunitaBelum ada peringkat
- Tibetan Buddhist approach to psychology and psychotherapyDokumen2 halamanTibetan Buddhist approach to psychology and psychotherapyCelia SteimanBelum ada peringkat
- A Simple Organizational Health ChecklistDokumen2 halamanA Simple Organizational Health Checklistdragonxyz70Belum ada peringkat
- ICD 10 Volume 2 en 2016Dokumen252 halamanICD 10 Volume 2 en 2016Bagas Andriyono100% (1)
- Bioplasm NLS User ManualDokumen136 halamanBioplasm NLS User ManualSun100% (1)
- COVID-19 Cytokine Storm Syndrome: Identification and TreatmentDokumen13 halamanCOVID-19 Cytokine Storm Syndrome: Identification and TreatmentIoana PelinBelum ada peringkat
- The Impact of COVID-19 in South AfricaDokumen6 halamanThe Impact of COVID-19 in South AfricaThe Wilson Center100% (10)
- Research On Genital HerpesDokumen2 halamanResearch On Genital HerpesTajuana Renee McCullough MartinBelum ada peringkat
- BSN 2ND YEAR 1ST SEMESTER FINAL 2021Dokumen20 halamanBSN 2ND YEAR 1ST SEMESTER FINAL 2021Alyanna TiglaoBelum ada peringkat
- Laporan Kimia Farma Maros 2 MeiDokumen14 halamanLaporan Kimia Farma Maros 2 MeiSitti AsiaBelum ada peringkat
- Care Advantage-Policy WordingDokumen61 halamanCare Advantage-Policy Wordingmilind.v.patilBelum ada peringkat
- NCM 113 - Lec Reviewer PrelimDokumen9 halamanNCM 113 - Lec Reviewer PrelimKylle AlimosaBelum ada peringkat
- Written Assignment Principles of Applied RehabilitationDokumen17 halamanWritten Assignment Principles of Applied RehabilitationRuqaiyah RahmanBelum ada peringkat
- Serwyn Rogers - q2 Project - Works CitedDokumen2 halamanSerwyn Rogers - q2 Project - Works Citedapi-495315809Belum ada peringkat
- EPIDEMIOLOGY LECTURE 4 Descriptive EpidemiologyDokumen37 halamanEPIDEMIOLOGY LECTURE 4 Descriptive EpidemiologylydiaBelum ada peringkat
- Tissue Adaptation To Physical Stress: A Proposed "Physical Stress Theory" To Guide Physical Therapist Practice, Education, and ResearchDokumen21 halamanTissue Adaptation To Physical Stress: A Proposed "Physical Stress Theory" To Guide Physical Therapist Practice, Education, and ResearchGavin Cao100% (1)
- Use of Ash and Mud For Handwashing in Low Income CommunitiesDokumen40 halamanUse of Ash and Mud For Handwashing in Low Income CommunitiesSTBM IndonesiaBelum ada peringkat
- Family Nursing Care PlanDokumen11 halamanFamily Nursing Care PlanBrenden Justin NarcisoBelum ada peringkat
- 2018 Philippine Health StatisticsDokumen224 halaman2018 Philippine Health StatisticsMark Angelo AquinoBelum ada peringkat
- Putrik 2014 - Access To RA BiologicsDokumen13 halamanPutrik 2014 - Access To RA BiologicsNona Delia ChiriacBelum ada peringkat
- LEPROSYDokumen55 halamanLEPROSYGeraldine Marie SalvoBelum ada peringkat
- Cu - Case Study FormatDokumen6 halamanCu - Case Study FormatJenny Turado Arbitrario67% (3)
- Health Insurance Ebook PDFDokumen29 halamanHealth Insurance Ebook PDFPrashant Pote100% (1)
- Kikuyu Medicinal PlantsDokumen15 halamanKikuyu Medicinal PlantsJoseph G Ngatia100% (2)
- Genetically Modified Products and Gene Therapy ReflectionDokumen1 halamanGenetically Modified Products and Gene Therapy ReflectionJosephine BautistaBelum ada peringkat