Anda mungkin juga menyukai
- Fsi GreekBasicCourse Volume1 StudentTextDokumen344 halamanFsi GreekBasicCourse Volume1 StudentTextbudapest1Belum ada peringkat
- Sample Opposition To Motion To Alter or Amend Judgment in United States District CourtDokumen3 halamanSample Opposition To Motion To Alter or Amend Judgment in United States District CourtStan BurmanBelum ada peringkat
- Pediatric Rehabilitation FiDokumen61 halamanPediatric Rehabilitation FifrakturhepatikaBelum ada peringkat
- Anecdotal Records For Piano Methods and Piano BooksDokumen5 halamanAnecdotal Records For Piano Methods and Piano BooksCes Disini-PitogoBelum ada peringkat
- Armor MagazineDokumen56 halamanArmor Magazine"Rufus"100% (2)
- Journal Pmed 1003787Dokumen20 halamanJournal Pmed 1003787GAYATHIRIBelum ada peringkat
- Vijay Law Series List of Publications - 2014: SN Subject/Title Publisher Year IsbnDokumen3 halamanVijay Law Series List of Publications - 2014: SN Subject/Title Publisher Year IsbnSabya Sachee Rai0% (2)
- A Study On Mistakes and Errors in Consecutive Interpretation From Vietnamese To English. Dang Huu Chinh. Qhf.1Dokumen38 halamanA Study On Mistakes and Errors in Consecutive Interpretation From Vietnamese To English. Dang Huu Chinh. Qhf.1Kavic100% (2)
- Barclays Global FX Quarterly Fed On Hold Eyes On GrowthDokumen42 halamanBarclays Global FX Quarterly Fed On Hold Eyes On GrowthgneymanBelum ada peringkat
- Functions of Communication Oral Communication PDFDokumen12 halamanFunctions of Communication Oral Communication PDFKrystle Francess Barrios0% (1)
- 10 11648 J Ijcd 20200301 13 PDFDokumen7 halaman10 11648 J Ijcd 20200301 13 PDFJosé Maria Chema Cari VillaBelum ada peringkat
- DiagnosisofpulmonaryTB in ChildrenDokumen8 halamanDiagnosisofpulmonaryTB in ChildrenSumit MitraBelum ada peringkat
- Research Article Toxoplasma Gondii Amongst Pregnant: Seroepidemiology of Women in Jazan Province, Saudi ArabiaDokumen7 halamanResearch Article Toxoplasma Gondii Amongst Pregnant: Seroepidemiology of Women in Jazan Province, Saudi ArabiaMAHFOUZ2015Belum ada peringkat
- Streptococcus Pneumoniae Carriage, Resistance and Serotypes Among Jordanian Children From Wadi Al Seer District, JordanDokumen8 halamanStreptococcus Pneumoniae Carriage, Resistance and Serotypes Among Jordanian Children From Wadi Al Seer District, JordanInternational Medical PublisherBelum ada peringkat
- Vih Actualizacion en OportunistasDokumen18 halamanVih Actualizacion en Oportunistassamuro625Belum ada peringkat
- Medicine - IJGMP - HUMAN IMMUNO DEFFICIENCY - Adetunji Oladeni Adeniji - NigeriaDokumen10 halamanMedicine - IJGMP - HUMAN IMMUNO DEFFICIENCY - Adetunji Oladeni Adeniji - Nigeriaiaset123Belum ada peringkat
- Nihpp rs3758745v1Dokumen20 halamanNihpp rs3758745v1Yulia Niswatul FauziyahBelum ada peringkat
- Jurnal Respi - Comparison of IGRA AssayDokumen5 halamanJurnal Respi - Comparison of IGRA AssaykaynabilBelum ada peringkat
- Fneur 04 00142Dokumen7 halamanFneur 04 00142nyuwwchocolavaBelum ada peringkat
- Sensitivity and Specificity of Typhoid Fever Rapid Antibody Tests For Laboratory Diagnosis at Two Sub-Saharan African SitesDokumen9 halamanSensitivity and Specificity of Typhoid Fever Rapid Antibody Tests For Laboratory Diagnosis at Two Sub-Saharan African SitesAde SupraptoBelum ada peringkat
- Respiratory Syncytial Virus Infections in Children With Acute Myeloid Leukemia: A Report From The Children's Oncology GroupDokumen3 halamanRespiratory Syncytial Virus Infections in Children With Acute Myeloid Leukemia: A Report From The Children's Oncology GrouperickmattosBelum ada peringkat
- Osman 2017Dokumen32 halamanOsman 2017Adrian Quiroga RodriguezBelum ada peringkat
- IGRA Vs PPDDokumen9 halamanIGRA Vs PPDrafaelreanoBelum ada peringkat
- Hepatitis B Virus (HBV) Infection Among Pregnant Women in Makurdi, NigeriaDokumen6 halamanHepatitis B Virus (HBV) Infection Among Pregnant Women in Makurdi, NigeriachaerunisautamiBelum ada peringkat
- Rubella Immunity in Women of Childbearing Age, Eight Years After The Immunization Program in IranDokumen3 halamanRubella Immunity in Women of Childbearing Age, Eight Years After The Immunization Program in IranCanda ArdityaBelum ada peringkat
- 24 PrabaDokumen9 halaman24 PrabaAbdul GhofurBelum ada peringkat
- 0148607115626921Dokumen8 halaman0148607115626921AndreannaBelum ada peringkat
- (Pro) Ing 1, Ada Kuesioner Juga12Dokumen8 halaman(Pro) Ing 1, Ada Kuesioner Juga12ilhamBelum ada peringkat
- Bulletin of The World Health OrganizationDokumen11 halamanBulletin of The World Health OrganizationJohn LewandowskiBelum ada peringkat
- Fatima's CommissionDokumen7 halamanFatima's CommissionSachie Daniela CheungBelum ada peringkat
- International Journal of Infectious DiseasesDokumen7 halamanInternational Journal of Infectious DiseasesyurikaBelum ada peringkat
- Cit230 PDFDokumen4 halamanCit230 PDFJoyBoyXBelum ada peringkat
- Diagnosing TB Infection in Children: Analysis of Discordances Using in Vitro Tests and The Tuberculin Skin TestDokumen9 halamanDiagnosing TB Infection in Children: Analysis of Discordances Using in Vitro Tests and The Tuberculin Skin TestAri Julian SaputraBelum ada peringkat
- Hyun Et Al. 2017 - Efficacy and Safety of TDF To Prevent MTCT of HBVDokumen13 halamanHyun Et Al. 2017 - Efficacy and Safety of TDF To Prevent MTCT of HBVizvery.badBelum ada peringkat
- Diagnosis and Treatment of Typhoid Fever and Associated PrevailingDokumen7 halamanDiagnosis and Treatment of Typhoid Fever and Associated Prevailing073090Belum ada peringkat
- TB in ChildrenDokumen9 halamanTB in Childrenparamita nindyaBelum ada peringkat
- Characterization of Bacterial Isolates Cultured From The Nasopharynx of Children With Sickle Cell Disease (SCD)Dokumen10 halamanCharacterization of Bacterial Isolates Cultured From The Nasopharynx of Children With Sickle Cell Disease (SCD)International Medical PublisherBelum ada peringkat
- MDR Somalia EID March 2013Dokumen3 halamanMDR Somalia EID March 2013hirsi200518Belum ada peringkat
- Comparative Study of Typhidot-M With Widal and Blood Culture in Diagnosis of Enteric FeverDokumen4 halamanComparative Study of Typhidot-M With Widal and Blood Culture in Diagnosis of Enteric FeverPranay BhosaleBelum ada peringkat
- Outcomes of HIV-infected Children With Tuberculosis Who Are Started On Antiretroviral Therapy in MalawiDokumen5 halamanOutcomes of HIV-infected Children With Tuberculosis Who Are Started On Antiretroviral Therapy in MalawiIrfan Dzakir NugrohoBelum ada peringkat
- Nej Mo A 0807381Dokumen12 halamanNej Mo A 0807381Mildred MontBelum ada peringkat
- Nej Mo A 1011214Dokumen11 halamanNej Mo A 1011214Debbi AnggrainiBelum ada peringkat
- BMC Public Health: Risk Factors For Pulmonary Tuberculosis: A Clinic-Based Case Control Study in The GambiaDokumen7 halamanBMC Public Health: Risk Factors For Pulmonary Tuberculosis: A Clinic-Based Case Control Study in The Gambiapuskesmas beloBelum ada peringkat
- High Virological Failure Rates in HIV1 Perinatally Infected Children in South Africa A Retrospective Cohort StudySouth African Medical JournalDokumen5 halamanHigh Virological Failure Rates in HIV1 Perinatally Infected Children in South Africa A Retrospective Cohort StudySouth African Medical JournalFarrell AnggoroBelum ada peringkat
- Dengue Infection During Pregnancy andDokumen7 halamanDengue Infection During Pregnancy andAlia SalviraBelum ada peringkat
- Tubex TestDokumen9 halamanTubex TestdnnivBelum ada peringkat
- Ijpa 18 93Dokumen7 halamanIjpa 18 93Frank Barreiro SanchezBelum ada peringkat
- Css Rizky Rafiqoh Afdin InggrisDokumen19 halamanCss Rizky Rafiqoh Afdin InggrisSyukri Be DeBelum ada peringkat
- Determinants of Neonatal Sepsis Among Neonates in The Northwest Part of Ethiopia: Case-Control StudyDokumen8 halamanDeterminants of Neonatal Sepsis Among Neonates in The Northwest Part of Ethiopia: Case-Control StudyNaman KhalidBelum ada peringkat
- Prevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalDokumen6 halamanPrevalence and Determinants of Human Immunodeficiency Virus and Tuberculosis Co-Infection at Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONBelum ada peringkat
- NXJDBSKHDDokumen4 halamanNXJDBSKHDMonika ZikraBelum ada peringkat
- Ijpedi2019 1054943Dokumen9 halamanIjpedi2019 1054943niaBelum ada peringkat
- SMW 2014 13935Dokumen6 halamanSMW 2014 13935Adi ParamarthaBelum ada peringkat
- Pharmacokinetics of anti-TB Drugs in Malawian Children: Reconsidering The Role of EthambutolDokumen6 halamanPharmacokinetics of anti-TB Drugs in Malawian Children: Reconsidering The Role of EthambutolIsmi Azisa Chaeria SaputriBelum ada peringkat
- Diagostic Efficacy OF Idirect Hemagglutiatio Test I Relatio To Kato Method For Diagosis of Schistosomiasis MasoiDokumen5 halamanDiagostic Efficacy OF Idirect Hemagglutiatio Test I Relatio To Kato Method For Diagosis of Schistosomiasis MasoiHebaHanyOmarBelum ada peringkat
- Fingerstick Gene TB DX - 240125 - 115659Dokumen10 halamanFingerstick Gene TB DX - 240125 - 115659Milenka JudithBelum ada peringkat
- Detection of Typhoid CarriersDokumen6 halamanDetection of Typhoid CarriersClarestaBelum ada peringkat
- Original Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodDokumen6 halamanOriginal Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodRidha Surya NugrahaBelum ada peringkat
- Impact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDokumen9 halamanImpact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDebby Astasya AnnisaBelum ada peringkat
- Jurnal Risk FX SepsisDokumen7 halamanJurnal Risk FX SepsiswilmaBelum ada peringkat
- Jurnal 2Dokumen12 halamanJurnal 2zingioBelum ada peringkat
- MorbiliDokumen7 halamanMorbilijourey08Belum ada peringkat
- 3 PDFDokumen8 halaman3 PDFriniBelum ada peringkat
- Prevalence and Associated Factors of HIV Infection Among Pregnant Women Attending Antenatal Care at The Yaoundé Central HospitalDokumen6 halamanPrevalence and Associated Factors of HIV Infection Among Pregnant Women Attending Antenatal Care at The Yaoundé Central HospitalnabilahbilqisBelum ada peringkat
- 1 - Incidence of Tuberculosis Meningitis in A High HIV Prevalence Serie de Caso 2018 (Modelo para o Trabalho)Dokumen9 halaman1 - Incidence of Tuberculosis Meningitis in A High HIV Prevalence Serie de Caso 2018 (Modelo para o Trabalho)SERGIO LOBATO FRANÇABelum ada peringkat
- Invasive Fungal Infections in Pediatric Oncology: MD MD MD MD MD MDDokumen6 halamanInvasive Fungal Infections in Pediatric Oncology: MD MD MD MD MD MDerickmattosBelum ada peringkat
- s41182 019 0162 9Dokumen8 halamans41182 019 0162 9Megan HarperBelum ada peringkat
- ManuscriptDokumen13 halamanManuscriptMegbaruBelum ada peringkat
- G6PD Deficiency Prevalence and Estimates of Affected Populations in Malaria Endemic Countries: A Geostatistical Model-Based MapDokumen101 halamanG6PD Deficiency Prevalence and Estimates of Affected Populations in Malaria Endemic Countries: A Geostatistical Model-Based MapfrakturhepatikaBelum ada peringkat
- Anestesi JurnalDokumen10 halamanAnestesi JurnalfrakturhepatikaBelum ada peringkat
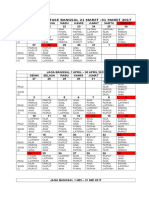
- Jadwal Jaga Stase Bangsal 21 Maret - 31 Maret 2017Dokumen4 halamanJadwal Jaga Stase Bangsal 21 Maret - 31 Maret 2017frakturhepatikaBelum ada peringkat
- Albumin Versus Other Fluids For Fluid Resuscitation in Patients With Sepsis: A Meta-AnalysisDokumen22 halamanAlbumin Versus Other Fluids For Fluid Resuscitation in Patients With Sepsis: A Meta-AnalysisfrakturhepatikaBelum ada peringkat
- Guidance For Intravenous Fluid and Electrolyte Prescription in AdultsDokumen8 halamanGuidance For Intravenous Fluid and Electrolyte Prescription in AdultsfrakturhepatikaBelum ada peringkat
- Basic and Advanced Cardiac Life Support: What's New?Dokumen6 halamanBasic and Advanced Cardiac Life Support: What's New?frakturhepatikaBelum ada peringkat
- S0149291812X00031 S0149291812001695 MainDokumen1 halamanS0149291812X00031 S0149291812001695 MainfrakturhepatikaBelum ada peringkat
- Aku BisaDokumen13 halamanAku BisafrakturhepatikaBelum ada peringkat
- RI Prelims GP H1 Paper 2 Ans KeyDokumen18 halamanRI Prelims GP H1 Paper 2 Ans Keyjaylynn6100% (1)
- Jataka Tales - The Crane and The CrabDokumen5 halamanJataka Tales - The Crane and The Crabshahrajan2k1Belum ada peringkat
- Superscope, Inc. v. Brookline Corp., Etc., Robert E. Lockwood, 715 F.2d 701, 1st Cir. (1983)Dokumen3 halamanSuperscope, Inc. v. Brookline Corp., Etc., Robert E. Lockwood, 715 F.2d 701, 1st Cir. (1983)Scribd Government DocsBelum ada peringkat
- Normalization Techniques For Multi-Criteria Decision Making: Analytical Hierarchy Process Case StudyDokumen11 halamanNormalization Techniques For Multi-Criteria Decision Making: Analytical Hierarchy Process Case StudyJohn GreenBelum ada peringkat
- Ila 0306Dokumen11 halamanIla 0306Hong ChenBelum ada peringkat
- Basa BasaDokumen4 halamanBasa Basamarilou sorianoBelum ada peringkat
- Jackson Et Al 2019 Using The Analytical Target Profile To Drive The Analytical Method LifecycleDokumen9 halamanJackson Et Al 2019 Using The Analytical Target Profile To Drive The Analytical Method LifecyclerbmoureBelum ada peringkat
- Magtajas vs. PryceDokumen3 halamanMagtajas vs. PryceRoyce PedemonteBelum ada peringkat
- Physics Waves MCQDokumen6 halamanPhysics Waves MCQAyan GhoshBelum ada peringkat
- Persona Core Poster - Creative Companion1 PDFDokumen1 halamanPersona Core Poster - Creative Companion1 PDFAdemola OgunlaluBelum ada peringkat
- CBSE Class11 Maths Notes 13 Limits and DerivativesDokumen7 halamanCBSE Class11 Maths Notes 13 Limits and DerivativesRoy0% (1)
- Computer Literacy Skills and Self-Efficacy Among Grade-12 - Computer System Servicing (CSS) StudentsDokumen25 halamanComputer Literacy Skills and Self-Efficacy Among Grade-12 - Computer System Servicing (CSS) StudentsNiwre Gumangan AguiwasBelum ada peringkat
- FR-A800 Plus For Roll To RollDokumen40 halamanFR-A800 Plus For Roll To RollCORTOCIRCUITANTEBelum ada peringkat
- Monograph SeismicSafetyDokumen63 halamanMonograph SeismicSafetyAlket DhamiBelum ada peringkat
- Anglicanism QuestionsDokumen36 halamanAnglicanism QuestionsspringsdanielconceptBelum ada peringkat
- Ingles Nivel 2Dokumen119 halamanIngles Nivel 2Perla Cortes100% (1)
- Position Paper Guns Dont Kill People Final DraftDokumen6 halamanPosition Paper Guns Dont Kill People Final Draftapi-273319954Belum ada peringkat
- Classics and The Atlantic Triangle - Caribbean Readings of Greece and Rome Via AfricaDokumen12 halamanClassics and The Atlantic Triangle - Caribbean Readings of Greece and Rome Via AfricaAleja KballeroBelum ada peringkat
- Chapter 1Dokumen16 halamanChapter 1MulugetaBelum ada peringkat
- Ron Clark ReflectionDokumen3 halamanRon Clark Reflectionapi-376753605Belum ada peringkat
- Boxnhl MBS (Design-D) Check SheetDokumen13 halamanBoxnhl MBS (Design-D) Check SheetKumari SanayaBelum ada peringkat
- Unit 1 - Identifying A Problem PDFDokumen16 halamanUnit 1 - Identifying A Problem PDFZanko FitnessBelum ada peringkat