Anda mungkin juga menyukai
- Heart & Lung: Ying Guo, MD, Wei Gao, MD, Hongxia Yang, MD, Cheng 'En Ma, MD, Shujian Sui, MDDokumen6 halamanHeart & Lung: Ying Guo, MD, Wei Gao, MD, Hongxia Yang, MD, Cheng 'En Ma, MD, Shujian Sui, MDnoviBelum ada peringkat
- Older Blood RBC StoredDokumen14 halamanOlder Blood RBC StoredPRADEEPBelum ada peringkat
- Does The Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and A Plea For Some Common SenseDokumen8 halamanDoes The Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and A Plea For Some Common SenseCris TianBelum ada peringkat
- Jurnal Kep KritisDokumen12 halamanJurnal Kep KritisRizal UmarBelum ada peringkat
- Silversides2017 Article ConservativeFluidManagementOrDDokumen18 halamanSilversides2017 Article ConservativeFluidManagementOrDDillaBelum ada peringkat
- Song 2014Dokumen11 halamanSong 2014Ayssa WitjaksonoBelum ada peringkat
- ContentServer AspDokumen14 halamanContentServer AspDeza Harati ZulfikarBelum ada peringkat
- Fiber TreatmentDokumen8 halamanFiber TreatmentLana AdilaBelum ada peringkat
- Jurnal BTKV DodiDokumen10 halamanJurnal BTKV DodiAchmad Dodi MeidiantoBelum ada peringkat
- 2017-Earlier Versus Later Initiation of Renal Replacement Therapy Among Critically Ill Patients With Acute Kidney Injury PDFDokumen14 halaman2017-Earlier Versus Later Initiation of Renal Replacement Therapy Among Critically Ill Patients With Acute Kidney Injury PDFClaudioLagosBelum ada peringkat
- Jain 2016 Defining The Role of UltrafiltratioDokumen9 halamanJain 2016 Defining The Role of UltrafiltratioAbdallah H. KamelBelum ada peringkat
- Lactated Ringer Solution Is Superior To Normal Saline Solution in Managing Acute PancreatitisDokumen7 halamanLactated Ringer Solution Is Superior To Normal Saline Solution in Managing Acute PancreatitisJulieth QuinteroBelum ada peringkat
- 2016 Article 1360Dokumen10 halaman2016 Article 1360Jesus Ernesto HernandezBelum ada peringkat
- Different Concentrations of Albumin Versus Crystalloid in PatientsDokumen11 halamanDifferent Concentrations of Albumin Versus Crystalloid in Patientsrleon746Belum ada peringkat
- Intermittent Vs Continuous Proton Pump Inhibitor Therapy For High-Risk Bleeding Ulcers - PMCDokumen1 halamanIntermittent Vs Continuous Proton Pump Inhibitor Therapy For High-Risk Bleeding Ulcers - PMCmuhammed barznjiBelum ada peringkat
- AmbulasiDokumen12 halamanAmbulasiRafii KhairuddinBelum ada peringkat
- Toscani2017 Article WhatIsTheImpactOfTheFluidChallDokumen12 halamanToscani2017 Article WhatIsTheImpactOfTheFluidChallNama ManaBelum ada peringkat
- Enteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsDokumen14 halamanEnteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsLea Bali Ulina SinurayaBelum ada peringkat
- Journal of Critical Care: Biao Wang, MD, Gang Chen, MD, Yifei Cao, MD, Jiping Xue, MD, Jia Li, MD, Yunfu Wu, MDDokumen5 halamanJournal of Critical Care: Biao Wang, MD, Gang Chen, MD, Yifei Cao, MD, Jiping Xue, MD, Jia Li, MD, Yunfu Wu, MDpramastutiBelum ada peringkat
- Sepsis - Eval and MGMTDokumen62 halamanSepsis - Eval and MGMTDr Ankit SharmaBelum ada peringkat
- Intermittent Vs Continuous Proton Pump Inhibitor Therapy For High-Risk Bleeding Ulcers A Systematic Review and Meta-AnalysisDokumen8 halamanIntermittent Vs Continuous Proton Pump Inhibitor Therapy For High-Risk Bleeding Ulcers A Systematic Review and Meta-AnalysisDaniel Hernandez QuinteroBelum ada peringkat
- Serum Albumin Level Adjusted With C-Reactive Protein Predicts Hemodialysis Patient SurvivalDokumen9 halamanSerum Albumin Level Adjusted With C-Reactive Protein Predicts Hemodialysis Patient Survivalmelda lestari haidirBelum ada peringkat
- Laparoscopic Versus Conventional Appendectomy - A Meta-Analysis of Randomized Controlled TrialsDokumen8 halamanLaparoscopic Versus Conventional Appendectomy - A Meta-Analysis of Randomized Controlled TrialsAdrian HaningBelum ada peringkat
- Chest: Does Central Venous Pressure Predict Fluid Responsiveness?Dokumen7 halamanChest: Does Central Venous Pressure Predict Fluid Responsiveness?ClaudioLagosBelum ada peringkat
- Quinolonas en Neumonia Nosocomial Un IsDokumen8 halamanQuinolonas en Neumonia Nosocomial Un IsIvan Ruiz HernandezBelum ada peringkat
- 1 RifDokumen29 halaman1 RifRifdah AmalinaBelum ada peringkat
- Anesth Analg-2012-Corcoran-640-51 PDFDokumen12 halamanAnesth Analg-2012-Corcoran-640-51 PDFBijay KCBelum ada peringkat
- Safety of Low-Molecular-Weight Heparin Compared To Unfractionated Heparin in Hemodialysis: A Systematic Review and Meta-AnalysisDokumen12 halamanSafety of Low-Molecular-Weight Heparin Compared To Unfractionated Heparin in Hemodialysis: A Systematic Review and Meta-AnalysisAaron GranadosBelum ada peringkat
- Early TIPS Versus Endoscopic Therapy For Secondary Prophylaxis After Management of Acute Esophageal Variceal Bleeding in Cirrhotic Patients: A Meta-Analysis of Randomized Controlled TrialsDokumen26 halamanEarly TIPS Versus Endoscopic Therapy For Secondary Prophylaxis After Management of Acute Esophageal Variceal Bleeding in Cirrhotic Patients: A Meta-Analysis of Randomized Controlled Trialsray liBelum ada peringkat
- Review 20 - 03 - 20 - 001Dokumen18 halamanReview 20 - 03 - 20 - 001Ulices QuintanaBelum ada peringkat
- Contoh Jurnal Meta AnalisisDokumen17 halamanContoh Jurnal Meta AnalisisMia Audina Miyanoshita100% (1)
- Academia and Clinic: Truth Survival in Clinical Research: An Evidence-Based Requiem?Dokumen8 halamanAcademia and Clinic: Truth Survival in Clinical Research: An Evidence-Based Requiem?Vlad PredaBelum ada peringkat
- Early Change in Platelet Count and MPV Levels of Patients Who Received Hemodialysis For The First Time Mogadishu Somalia ExperienceDokumen5 halamanEarly Change in Platelet Count and MPV Levels of Patients Who Received Hemodialysis For The First Time Mogadishu Somalia ExperienceDea Fiesta JatikusumaBelum ada peringkat
- 2017 Article 605Dokumen11 halaman2017 Article 605UswatunnisaBelum ada peringkat
- 10 1016@j Clinthera 2020 01 008Dokumen19 halaman10 1016@j Clinthera 2020 01 008skripsi kapBelum ada peringkat
- Farmakopunktur Pada KankerDokumen15 halamanFarmakopunktur Pada KankerYoshua ViventiusBelum ada peringkat
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalDari EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalBelum ada peringkat
- Low-Versus High-Chloride Content Intravenous Solutions For Critically Ill and Perioperative Adult Patients: A Systematic Review and Meta-AnalysisDokumen9 halamanLow-Versus High-Chloride Content Intravenous Solutions For Critically Ill and Perioperative Adult Patients: A Systematic Review and Meta-AnalysisAlexandre CavalcantiBelum ada peringkat
- Dialyzer Membrane Permeability and Survi PDFDokumen7 halamanDialyzer Membrane Permeability and Survi PDFNurul SaufikaBelum ada peringkat
- Noninvasive Monitoring 2016Dokumen6 halamanNoninvasive Monitoring 2016Maria LaiaBelum ada peringkat
- Piis0149291815001484 PDFDokumen10 halamanPiis0149291815001484 PDFWarunee MingpunBelum ada peringkat
- Journal Pre-Proofs: Diabetes Research and Clinical PracticeDokumen35 halamanJournal Pre-Proofs: Diabetes Research and Clinical PracticeAzmafiBelum ada peringkat
- HES Pada SepsisDokumen8 halamanHES Pada Sepsisvanadiel4Belum ada peringkat
- Tight Glycemic Control in Critically Ill PediatricDokumen11 halamanTight Glycemic Control in Critically Ill Pediatricbella friscaamaliaBelum ada peringkat
- Araujo 2015Dokumen9 halamanAraujo 2015Omar SolisBelum ada peringkat
- The Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsDokumen9 halamanThe Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsLucky PratamaBelum ada peringkat
- Art2 HT3Dokumen3 halamanArt2 HT3Glenda MaríaBelum ada peringkat
- MPV SciDokumen6 halamanMPV SciMikael AngelooBelum ada peringkat
- Efficacy of Red Blood Cell Transfusion in The Critically Ill (Original Article)Dokumen8 halamanEfficacy of Red Blood Cell Transfusion in The Critically Ill (Original Article)Rayhan OemarBelum ada peringkat
- HDFVVC EfectoDokumen11 halamanHDFVVC Efectogiseladelarosa2006Belum ada peringkat
- Top Trials in Gastroenterology & Hepatology, 2nd EditionDari EverandTop Trials in Gastroenterology & Hepatology, 2nd EditionBelum ada peringkat
- Pone 0062323Dokumen10 halamanPone 0062323Malik IbrahimBelum ada peringkat
- Early Management of Acute Pancreatitis-A Review of The Best Evidence. Dig Liver Dis 2017Dokumen32 halamanEarly Management of Acute Pancreatitis-A Review of The Best Evidence. Dig Liver Dis 2017América FloresBelum ada peringkat
- Quick guide to Laboratory Medicine: a student's overviewDari EverandQuick guide to Laboratory Medicine: a student's overviewBelum ada peringkat
- Clinical ResearchDokumen13 halamanClinical ResearchkarmilaBelum ada peringkat
- Heterogeneity of Terminology and Clinical Definitions in Adult Idiopathic Thrombocytopenic Purpura: A Critical Appraisal From Literature AnalysisDokumen4 halamanHeterogeneity of Terminology and Clinical Definitions in Adult Idiopathic Thrombocytopenic Purpura: A Critical Appraisal From Literature AnalysisVladimir Henry Triguero RosalesBelum ada peringkat
- Puskarich 2014Dokumen6 halamanPuskarich 2014Martha AcevesBelum ada peringkat
- Cherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyDokumen10 halamanCherukuri Et Al. 2018 - Home Haemodialysis Treatment and Outcomes, Retrospective Analysis of KIHDNEyShareDialysisBelum ada peringkat
- Review Dysphagia Tto PoststrokeDokumen7 halamanReview Dysphagia Tto PoststrokeTrinidad OdaeBelum ada peringkat
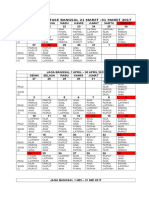
- Jadwal Jaga Stase Bangsal 21 Maret - 31 Maret 2017Dokumen4 halamanJadwal Jaga Stase Bangsal 21 Maret - 31 Maret 2017frakturhepatikaBelum ada peringkat
- Anestesi JurnalDokumen10 halamanAnestesi JurnalfrakturhepatikaBelum ada peringkat
- G6PD Deficiency Prevalence and Estimates of Affected Populations in Malaria Endemic Countries: A Geostatistical Model-Based MapDokumen101 halamanG6PD Deficiency Prevalence and Estimates of Affected Populations in Malaria Endemic Countries: A Geostatistical Model-Based MapfrakturhepatikaBelum ada peringkat
- Guidance For Intravenous Fluid and Electrolyte Prescription in AdultsDokumen8 halamanGuidance For Intravenous Fluid and Electrolyte Prescription in AdultsfrakturhepatikaBelum ada peringkat
- TugasDokumen4 halamanTugasfrakturhepatikaBelum ada peringkat
- Basic and Advanced Cardiac Life Support: What's New?Dokumen6 halamanBasic and Advanced Cardiac Life Support: What's New?frakturhepatikaBelum ada peringkat
- Pediatric Rehabilitation FiDokumen61 halamanPediatric Rehabilitation FifrakturhepatikaBelum ada peringkat
- Aku BisaDokumen13 halamanAku BisafrakturhepatikaBelum ada peringkat
- S0149291812X00031 S0149291812001695 MainDokumen1 halamanS0149291812X00031 S0149291812001695 MainfrakturhepatikaBelum ada peringkat
- Bche 4090 1155168548Dokumen7 halamanBche 4090 1155168548Yenny TsaiBelum ada peringkat
- Ophthalmology PDFDokumen92 halamanOphthalmology PDFMarwa AhmedBelum ada peringkat
- Summative Test-G8-Quarter-4Dokumen13 halamanSummative Test-G8-Quarter-4Charmaine CanonoBelum ada peringkat
- Cardio CaseDokumen21 halamanCardio CaseJan Rae Y. BattungBelum ada peringkat
- Fluids and Transport: Fundamentals of Anatomy & PhysiologyDokumen161 halamanFluids and Transport: Fundamentals of Anatomy & Physiologyann aquinoBelum ada peringkat
- HSCRP Level-0,5Dokumen10 halamanHSCRP Level-0,5Nova SipahutarBelum ada peringkat
- Brigada EskwelaDokumen35 halamanBrigada EskwelaRichard Panaguiton CanlasBelum ada peringkat
- 11 Chapter 1Dokumen49 halaman11 Chapter 1ram6025Belum ada peringkat
- Cancer Case StudyDokumen15 halamanCancer Case StudyRobin HaliliBelum ada peringkat
- Neonatal JaundiceDokumen56 halamanNeonatal Jaundicesuardiman acoBelum ada peringkat
- Newport, D.J. and Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. Cognitive Neuroscience JAARTALDokumen8 halamanNewport, D.J. and Nemeroff, C.B. Neurobiology of Posttraumatic Stress Disorder. Cognitive Neuroscience JAARTALg10564433Belum ada peringkat
- The Truth About Lie Detectors Aka Polygraph TestsDokumen4 halamanThe Truth About Lie Detectors Aka Polygraph TestsMălina-Ionela CorlătianuBelum ada peringkat
- Australian Prescriber (1988) Bioavailability and First Past ClearanceDokumen3 halamanAustralian Prescriber (1988) Bioavailability and First Past Clearance1234chocoBelum ada peringkat
- Lesson 4 - Circulatory SystemDokumen21 halamanLesson 4 - Circulatory Systemapi-307592530Belum ada peringkat
- Urine Volatile Organic Compounds As Biomarkers For Minimal Change Type Nephrotic SyndromeDokumen24 halamanUrine Volatile Organic Compounds As Biomarkers For Minimal Change Type Nephrotic SyndromeYasser AlghrafyBelum ada peringkat
- Format Ketikan LabDokumen9 halamanFormat Ketikan Labapril babyBelum ada peringkat
- Golnic Lipidai Fingernails 000029915Dokumen9 halamanGolnic Lipidai Fingernails 000029915Vita BūdvytėBelum ada peringkat
- Uropati ObstruktifDokumen22 halamanUropati ObstruktifEvan Permana100% (1)
- Patente Endoesqueleto para Sex Doll SiliconaDokumen12 halamanPatente Endoesqueleto para Sex Doll SiliconaGabriel De Jesus100% (1)
- 22 Stretches To Improve Your Flexibility For PoleDokumen10 halaman22 Stretches To Improve Your Flexibility For PoleSarah86% (7)
- EMG Methods For Evaluating Muscle and Nerve FunctionDokumen546 halamanEMG Methods For Evaluating Muscle and Nerve Function4569077100% (1)
- Cell Types SeDokumen16 halamanCell Types SeKendallBelum ada peringkat
- Complex Anorectal Disorders PDFDokumen817 halamanComplex Anorectal Disorders PDFGabriela Balan100% (2)
- Adult Health Final Study GuideDokumen5 halamanAdult Health Final Study GuideNurseNancy93100% (1)
- Oriflamebeautyacademy SkincareDokumen173 halamanOriflamebeautyacademy Skincareapi-37629474750% (2)
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDokumen5 halamanPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralBelum ada peringkat
- (Criminalistics 5) Police Polygraphy (Lie-Detection)Dokumen15 halaman(Criminalistics 5) Police Polygraphy (Lie-Detection)Yam P Bustamante100% (2)
- II. Blood Vessels Physiology By: Dr. Abdulrahman Aqra MD MSCDokumen12 halamanII. Blood Vessels Physiology By: Dr. Abdulrahman Aqra MD MSCapi-290338101Belum ada peringkat
- Circadian RhythmsDokumen4 halamanCircadian Rhythmsapi-642709499Belum ada peringkat
- Occult Meaning of Colours Purple Haze, All in My BrainDokumen54 halamanOccult Meaning of Colours Purple Haze, All in My BrainrobinhoodlumBelum ada peringkat