Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Activity Design ScoutingDokumen10 halamanActivity Design ScoutingHoneyjo Nette100% (9)
- Geo Lab Report Point LoadDokumen9 halamanGeo Lab Report Point Loaddrbrainsol50% (2)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- 8 DaysDokumen337 halaman8 Daysprakab100% (1)
- Lindsay: VasquezDokumen1 halamanLindsay: Vasquezapi-240028260Belum ada peringkat
- Bullying IncivilitynovoiceDokumen14 halamanBullying Incivilitynovoiceapi-240028260Belum ada peringkat
- Project Final ReportDokumen13 halamanProject Final Reportapi-240028260Belum ada peringkat
- Service Learningnurs450Dokumen7 halamanService Learningnurs450api-240028260Belum ada peringkat
- Nurs 300 PortfolioDokumen2 halamanNurs 300 Portfolioapi-240028260Belum ada peringkat
- L Vasqueznurs340vulnerablepopulationDokumen6 halamanL Vasqueznurs340vulnerablepopulationapi-240028260Belum ada peringkat
- Ctu Medication ManagementnovoiceDokumen12 halamanCtu Medication Managementnovoiceapi-240028260Belum ada peringkat
- Vasquez L Nurs310-RealageDokumen11 halamanVasquez L Nurs310-Realageapi-240028260Belum ada peringkat
- Service Learningno VoiceDokumen8 halamanService Learningno Voiceapi-240028260Belum ada peringkat
- Osp Step 2Dokumen3 halamanOsp Step 2api-240028260Belum ada peringkat
- Running Head: Scope and Standards of Practice 1Dokumen11 halamanRunning Head: Scope and Standards of Practice 1api-240028260Belum ada peringkat
- Nurs 324 Discussion Post Dated 1Dokumen2 halamanNurs 324 Discussion Post Dated 1api-240028260Belum ada peringkat
- Patricia Benner: Brianna Rich Denise Preston Lindsay Vasquez Nursing 324 Ferris State UniversityDokumen9 halamanPatricia Benner: Brianna Rich Denise Preston Lindsay Vasquez Nursing 324 Ferris State Universityapi-240028260Belum ada peringkat
- L Vasquez AnalyzingaleaderDokumen11 halamanL Vasquez Analyzingaleaderapi-240028260Belum ada peringkat
- CaseDokumen2 halamanCaseapi-240028260Belum ada peringkat
- My Ethical ProfileDokumen7 halamanMy Ethical Profileapi-240028260Belum ada peringkat
- Oral HealthDokumen2 halamanOral Healthapi-240028260Belum ada peringkat
- Group 7 EncouragingexerciseDokumen13 halamanGroup 7 Encouragingexerciseapi-240028260Belum ada peringkat
- Vasquez HP ToolDokumen6 halamanVasquez HP Toolapi-240028260Belum ada peringkat
- BSN ChecklistDokumen1 halamanBSN Checklistapi-306305343Belum ada peringkat
- 5.mpob - LeadershipDokumen21 halaman5.mpob - LeadershipChaitanya PillalaBelum ada peringkat
- Navid DDLDokumen7 halamanNavid DDLVaibhav KarambeBelum ada peringkat
- Capitalism Communism Socialism DebateDokumen28 halamanCapitalism Communism Socialism DebateMr. Graham Long100% (1)
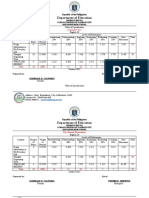
- Table of Specification ENGLISHDokumen2 halamanTable of Specification ENGLISHDonn Abel Aguilar IsturisBelum ada peringkat
- Proportions PosterDokumen1 halamanProportions Posterapi-214764900Belum ada peringkat
- Embedded Systems - RTOSDokumen23 halamanEmbedded Systems - RTOSCheril MehtaBelum ada peringkat
- How To Prepare Squash Specimen Samples For Microscopic ObservationDokumen3 halamanHow To Prepare Squash Specimen Samples For Microscopic ObservationSAMMYBelum ada peringkat
- A Personality Trait-Based Interactionist Model of Job PerformanceDokumen18 halamanA Personality Trait-Based Interactionist Model of Job PerformanceAlvina AhmedBelum ada peringkat
- Backup 2Dokumen59 halamanBackup 2Fabiola Tineo GamarraBelum ada peringkat
- DEMO 2 Critical Reading As ReasoningDokumen3 halamanDEMO 2 Critical Reading As ReasoningConnieRoseRamosBelum ada peringkat
- Mitchell 1986Dokumen34 halamanMitchell 1986Sara Veronica Florentin CuencaBelum ada peringkat
- NMIMS MBA Midterm Decision Analysis and Modeling ExamDokumen2 halamanNMIMS MBA Midterm Decision Analysis and Modeling ExamSachi SurbhiBelum ada peringkat
- COS1512 202 - 2015 - 1 - BDokumen33 halamanCOS1512 202 - 2015 - 1 - BLina Slabbert-van Der Walt100% (1)
- Charny - Mathematical Models of Bioheat TransferDokumen137 halamanCharny - Mathematical Models of Bioheat TransferMadalena PanBelum ada peringkat
- Rolfsen Knot Table Guide Crossings 1-10Dokumen4 halamanRolfsen Knot Table Guide Crossings 1-10Pangloss LeibnizBelum ada peringkat
- Outgoing Call Block BroadcastReceiver ExampleDokumen3 halamanOutgoing Call Block BroadcastReceiver ExampleZainUlAbidinBelum ada peringkat
- Viola Jones AlgorithmDokumen4 halamanViola Jones AlgorithmBhumika GowdaBelum ada peringkat
- Math Curriculum Overview Grades 1 8Dokumen1 halamanMath Curriculum Overview Grades 1 8GuiselleBelum ada peringkat
- Significance of Vaiseshika's PragabhavaDokumen5 halamanSignificance of Vaiseshika's Pragabhavavskanchi0% (1)
- Dompet Digital Di Kota SemarangDokumen10 halamanDompet Digital Di Kota SemarangRikson TandelilinBelum ada peringkat
- NAVMC 3500.35A (Food Services)Dokumen88 halamanNAVMC 3500.35A (Food Services)Alexander HawkBelum ada peringkat
- Rhythm Music and Education - Dalcroze PDFDokumen409 halamanRhythm Music and Education - Dalcroze PDFJhonatas Carmo100% (3)
- Cost of Litigation Report (2015)Dokumen17 halamanCost of Litigation Report (2015)GlennKesslerWPBelum ada peringkat
- McCann MIA CredentialsDokumen20 halamanMcCann MIA CredentialsgbertainaBelum ada peringkat
- Relay Testing Management SoftwareDokumen10 halamanRelay Testing Management Softwarechichid2008Belum ada peringkat
- Saline Water Intrusion in Coastal Aquifers: A Case Study From BangladeshDokumen6 halamanSaline Water Intrusion in Coastal Aquifers: A Case Study From BangladeshIOSRJEN : hard copy, certificates, Call for Papers 2013, publishing of journalBelum ada peringkat
- Google Fusion Tables: A Case StudyDokumen4 halamanGoogle Fusion Tables: A Case StudySeanBelum ada peringkat