Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Form PL-2 Application GuideDokumen2 halamanForm PL-2 Application GuideMelin w. Abad67% (6)
- Classwork Notes and Pointers Statutory Construction - TABORDA, CHRISTINE ANNDokumen47 halamanClasswork Notes and Pointers Statutory Construction - TABORDA, CHRISTINE ANNChristine Ann TabordaBelum ada peringkat
- RFID Sticker and and Card Replacement 2019 PDFDokumen1 halamanRFID Sticker and and Card Replacement 2019 PDFJessamyn DimalibotBelum ada peringkat
- C - TS4CO - 2021: There Are 2 Correct Answers To This QuestionDokumen54 halamanC - TS4CO - 2021: There Are 2 Correct Answers To This QuestionHclementeBelum ada peringkat
- Latte Da MenuDokumen1 halamanLatte Da Menuapi-302325078Belum ada peringkat
- Latte Da FinalDokumen41 halamanLatte Da Finalapi-302325078Belum ada peringkat
- 4 DollarsperdayassignmentDokumen18 halaman4 Dollarsperdayassignmentapi-302325078Belum ada peringkat
- Untitleddocument 3Dokumen9 halamanUntitleddocument 3api-302325078Belum ada peringkat
- 34g/L AA, 150 G/L Dex, 27.5 G/L IL at 75ml/hr X 24 HrsDokumen4 halaman34g/L AA, 150 G/L Dex, 27.5 G/L IL at 75ml/hr X 24 Hrsapi-302325078Belum ada peringkat
- AdimeoralcancerDokumen2 halamanAdimeoralcancerapi-302325078Belum ada peringkat
- Adimecf 1Dokumen3 halamanAdimecf 1api-302325078Belum ada peringkat
- Roughpersonalstatement 3 Nutr 494Dokumen3 halamanRoughpersonalstatement 3 Nutr 494api-302325078Belum ada peringkat
- Arcmap and PythonDokumen29 halamanArcmap and PythonMiguel AngelBelum ada peringkat
- Jurnal Manajemen IndonesiaDokumen20 halamanJurnal Manajemen IndonesiaThoriq MBelum ada peringkat
- 2nd YearDokumen5 halaman2nd YearAnbalagan GBelum ada peringkat
- Business Planning Process: Chapter-Four Operations Planning and ControlDokumen12 halamanBusiness Planning Process: Chapter-Four Operations Planning and ControlGemechis BussaBelum ada peringkat
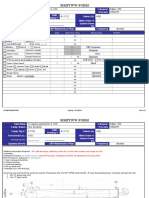
- Simptww S-1105Dokumen3 halamanSimptww S-1105Vijay RajaindranBelum ada peringkat
- Polisomnografí A Dinamica No Dise.: Club de Revistas Julián David Cáceres O. OtorrinolaringologíaDokumen25 halamanPolisomnografí A Dinamica No Dise.: Club de Revistas Julián David Cáceres O. OtorrinolaringologíaDavid CáceresBelum ada peringkat
- MAY-2006 International Business Paper - Mumbai UniversityDokumen2 halamanMAY-2006 International Business Paper - Mumbai UniversityMAHENDRA SHIVAJI DHENAKBelum ada peringkat
- Brochure - Coming To Work in The Netherlands (2022)Dokumen16 halamanBrochure - Coming To Work in The Netherlands (2022)Tshifhiwa MathivhaBelum ada peringkat
- Other Project Content-1 To 8Dokumen8 halamanOther Project Content-1 To 8Amit PasiBelum ada peringkat
- Senarai Syarikat Berdaftar MidesDokumen6 halamanSenarai Syarikat Berdaftar Midesmohd zulhazreen bin mohd nasirBelum ada peringkat
- Understanding Learning Theories and Knowledge AcquisitionDokumen38 halamanUnderstanding Learning Theories and Knowledge AcquisitionKarl Maloney Erfe100% (1)
- Lab 5: Conditional probability and contingency tablesDokumen6 halamanLab 5: Conditional probability and contingency tablesmlunguBelum ada peringkat
- Kenneth L. Campbell - The History of Britain and IrelandDokumen505 halamanKenneth L. Campbell - The History of Britain and IrelandKseniaBelum ada peringkat
- A COIN FOR A BETTER WILDLIFEDokumen8 halamanA COIN FOR A BETTER WILDLIFEDragomir DanielBelum ada peringkat
- AReviewof Environmental Impactof Azo Dyes International PublicationDokumen18 halamanAReviewof Environmental Impactof Azo Dyes International PublicationPvd CoatingBelum ada peringkat
- Adam Smith Abso Theory - PDF Swati AgarwalDokumen3 halamanAdam Smith Abso Theory - PDF Swati AgarwalSagarBelum ada peringkat
- Batman Vs Riddler RiddlesDokumen3 halamanBatman Vs Riddler RiddlesRoy Lustre AgbonBelum ada peringkat
- Introduction To Competitor AnalysisDokumen18 halamanIntroduction To Competitor AnalysisSrinivas NandikantiBelum ada peringkat
- WAS Argumentative EssayDokumen4 halamanWAS Argumentative EssayJandresBelum ada peringkat
- Lesson Plan Maam MyleenDokumen7 halamanLesson Plan Maam MyleenRochelle RevadeneraBelum ada peringkat
- Dues & Scholarship Section: NotificationDokumen6 halamanDues & Scholarship Section: NotificationMUNEEB WAHEEDBelum ada peringkat
- Product Manual: Control Cabinet M2001Dokumen288 halamanProduct Manual: Control Cabinet M2001openid_6qpqEYklBelum ada peringkat
- Iron FoundationsDokumen70 halamanIron FoundationsSamuel Laura HuancaBelum ada peringkat
- Portfolio ValuationDokumen1 halamanPortfolio ValuationAnkit ThakreBelum ada peringkat
- Category Theory For Programmers by Bartosz MilewskiDokumen565 halamanCategory Theory For Programmers by Bartosz MilewskiJohn DowBelum ada peringkat
- Ten Lessons (Not?) Learnt: Asset AllocationDokumen30 halamanTen Lessons (Not?) Learnt: Asset AllocationkollingmBelum ada peringkat