Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Volunteer HoursDokumen1 halamanVolunteer Hoursapi-310375757Belum ada peringkat
- Bad Choice at MemorialDokumen17 halamanBad Choice at Memorialapi-310375757Belum ada peringkat
- Engl 310Dokumen6 halamanEngl 310api-310375757Belum ada peringkat
- Final ProjectDokumen7 halamanFinal Projectapi-310375757Belum ada peringkat
- Hourly Rounding and The Effects On Patient Safety and Satisfaction ArtifactDokumen29 halamanHourly Rounding and The Effects On Patient Safety and Satisfaction Artifactapi-310375757Belum ada peringkat
- WileycancerDokumen11 halamanWileycancerapi-310375757Belum ada peringkat
- Artifact FinalDokumen8 halamanArtifact Finalapi-310375757Belum ada peringkat
- Parents BewareDokumen8 halamanParents Bewareapi-310375757Belum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Oral Manifestations of Connective Tissue Disease (CTDDokumen34 halamanOral Manifestations of Connective Tissue Disease (CTDFatin Nabihah Jamil67% (3)
- HCP EngDokumen109 halamanHCP Engclap smrBelum ada peringkat
- IFIC Basic Concepts of Infection ControlDokumen196 halamanIFIC Basic Concepts of Infection ControlYULI22280% (5)
- Approach To in Born Errors of MetabolismDokumen112 halamanApproach To in Born Errors of MetabolismGurpreet Singh100% (3)
- You Dont Know JackDokumen7 halamanYou Dont Know JackSunaira MalikBelum ada peringkat
- Therapeutic Management of Laryngectomy - PDF / KUNNAMPALLIL GEJO JOHNDokumen31 halamanTherapeutic Management of Laryngectomy - PDF / KUNNAMPALLIL GEJO JOHNKUNNAMPALLIL GEJO JOHNBelum ada peringkat
- Ranger Medic Handbook Draft 2003 - 1Dokumen110 halamanRanger Medic Handbook Draft 2003 - 1flightmedic71100% (1)
- Care Map UtiDokumen1 halamanCare Map UtiJonathonBelum ada peringkat
- Director Quality Risk Management in Western MA Resume Stanley KoniecznyDokumen2 halamanDirector Quality Risk Management in Western MA Resume Stanley KoniecznyStanley KoniecznyBelum ada peringkat
- Differential Diagnosis of Acute Exacerbation of CopdDokumen4 halamanDifferential Diagnosis of Acute Exacerbation of CopdManik ParmeliaBelum ada peringkat
- What Is Medical Marijuana?Dokumen8 halamanWhat Is Medical Marijuana?Dragoș TiculaBelum ada peringkat
- Disseminated Intravascular Coagulopathy Dic 1 1Dokumen25 halamanDisseminated Intravascular Coagulopathy Dic 1 1api-394684626Belum ada peringkat
- Fissure Treatment in MumbaiDokumen4 halamanFissure Treatment in MumbaiSambit ClinicBelum ada peringkat
- Nawrin JahanDokumen82 halamanNawrin JahanMamanya Fadhil HaniBelum ada peringkat
- ADA Guidelines For Infection Control 3rd EdDokumen56 halamanADA Guidelines For Infection Control 3rd Edaprmaster100% (2)
- Lap InstrumentsDokumen7 halamanLap InstrumentskhaleeltahaBelum ada peringkat
- EE372 Biomedical InstrumentationDokumen2 halamanEE372 Biomedical InstrumentationDeepu V SBelum ada peringkat
- Theories Frameworks and ModelsDokumen33 halamanTheories Frameworks and ModelsJaysonPangilinanAbanBelum ada peringkat
- Introduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologyDokumen26 halamanIntroduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologymochkurniawanBelum ada peringkat
- Potts Disease NCP .. JustificationDokumen8 halamanPotts Disease NCP .. JustificationMicah SalesBelum ada peringkat
- Woodcutters TechniqueDokumen3 halamanWoodcutters TechniqueToo SmallBelum ada peringkat
- Medical CenterDokumen38 halamanMedical CenterKhea Micole MayBelum ada peringkat
- What Are Moral DilemmasDokumen7 halamanWhat Are Moral DilemmasMary Anne Rocafor NaelgasBelum ada peringkat
- Product Monograph - Zoledronic Acid For Injection ConcentrateDokumen58 halamanProduct Monograph - Zoledronic Acid For Injection ConcentrateMisgi Candra DasaBelum ada peringkat
- Control of Blood Glucose LevelDokumen21 halamanControl of Blood Glucose LevelalynnsakinaBelum ada peringkat
- PGHHHMDokumen30 halamanPGHHHMDaipayan Lodh75% (4)
- ORTHOSIS - and ProthesisDokumen112 halamanORTHOSIS - and Prothesismanjukumard2007100% (1)
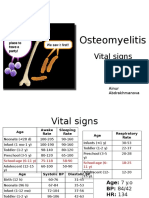
- PBL 2 - OsteomyelitisDokumen10 halamanPBL 2 - OsteomyelitisAinur AbdrakhmanovaBelum ada peringkat
- Lecture 1 Introduction To The Course and History of PharmacyDokumen19 halamanLecture 1 Introduction To The Course and History of Pharmacyahusain100% (1)
- Jaw LashDokumen16 halamanJaw LashSven BivalBelum ada peringkat