Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- NCPDokumen3 halamanNCPWendy EscalanteBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Nasogastric Tube Management and CareDokumen21 halamanNasogastric Tube Management and CareWendy EscalanteBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- NCP 2 MiDokumen16 halamanNCP 2 MiWendy EscalanteBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Drug StudyDokumen14 halamanDrug StudyWendy EscalanteBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Assessment of Kidneys PDFDokumen1 halamanAssessment of Kidneys PDFWendy EscalanteBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Assessment of KidneysDokumen1 halamanAssessment of KidneysWendy EscalanteBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Caring For The Bedridden PatientDokumen1 halamanCaring For The Bedridden PatientWendy EscalanteBelum ada peringkat
- PATHODokumen2 halamanPATHOWendy EscalanteBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
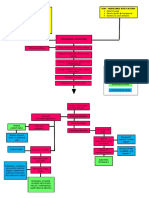
- Modifiable Risk Factors Non - Modifiable Risk Factors: LegendDokumen2 halamanModifiable Risk Factors Non - Modifiable Risk Factors: LegendWendy Escalante100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- 02 Orig Art 02 PDFDokumen3 halaman02 Orig Art 02 PDFWendy EscalanteBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Degenerative Joint DiseaseDokumen35 halamanDegenerative Joint DiseaseWendy EscalanteBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Pediatric NursingDokumen16 halamanPediatric NursingWendy Escalante100% (1)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Concept Map of Carotid Artery DiseaseDokumen2 halamanConcept Map of Carotid Artery DiseaseWendy EscalanteBelum ada peringkat
- Acid-Ash DietDokumen10 halamanAcid-Ash DietWendy Escalante0% (1)
- Concept Map of CKD Gastrointestinal SymptomsDokumen4 halamanConcept Map of CKD Gastrointestinal SymptomsWendy Escalante0% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Brat DietDokumen8 halamanBrat DietWendy EscalanteBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- At DietDokumen8 halamanAt DietWendy EscalanteBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Fundamentals in NursingDokumen9 halamanFundamentals in NursingWendy EscalanteBelum ada peringkat
- DM Report1Dokumen16 halamanDM Report1Wendy EscalanteBelum ada peringkat
- Drug Study FinalDokumen8 halamanDrug Study FinalWendy EscalanteBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Case Presentation: Group 2Dokumen30 halamanCase Presentation: Group 2Wendy EscalanteBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Therapeutic DietDokumen3 halamanTherapeutic DietWendy EscalanteBelum ada peringkat
- Diabetes MellitusDokumen5 halamanDiabetes MellitusWendy EscalanteBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDokumen78 halamanIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsWendy EscalanteBelum ada peringkat
- FNCP CommunityDokumen4 halamanFNCP CommunityWendy EscalanteBelum ada peringkat
- Nursing Care For Patient With Neurological DiseaseDokumen8 halamanNursing Care For Patient With Neurological DiseaseWendy EscalanteBelum ada peringkat
- Eating DisordersDokumen238 halamanEating DisordersIldikó Márton100% (5)
- Phobias Phobias PhobiasDokumen2 halamanPhobias Phobias PhobiasMhae ShahBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Quotes by Milton EricksonDokumen2 halamanQuotes by Milton Ericksongiovana14Belum ada peringkat
- OCD and Psychological ManagementDokumen35 halamanOCD and Psychological ManagementhelalBelum ada peringkat
- Child and Adolescent Psychiatric Assessment (CAPA) - Child InterviewDokumen210 halamanChild and Adolescent Psychiatric Assessment (CAPA) - Child InterviewVicki B VeeBelum ada peringkat
- Beck Depression Inventory ScoringDokumen2 halamanBeck Depression Inventory ScoringFaranBelum ada peringkat
- A Beautiful Mind Schziophrenia Case Study (Movie Review)Dokumen4 halamanA Beautiful Mind Schziophrenia Case Study (Movie Review)Ermela Casillar EspinoBelum ada peringkat
- ToR - Child Safeguarding Specialist (Updated)Dokumen9 halamanToR - Child Safeguarding Specialist (Updated)Milykhia Ngouabi McKenzie-WeekesBelum ada peringkat
- The Social Construction and Reframing of ADHDDokumen13 halamanThe Social Construction and Reframing of ADHDJustin M.100% (1)
- What Are The Signs of AutismDokumen2 halamanWhat Are The Signs of AutismDenver SignabenBelum ada peringkat
- Elementary School Students' Mental Health During The CoronaVirus Pandemic (COVID-19)Dokumen13 halamanElementary School Students' Mental Health During The CoronaVirus Pandemic (COVID-19)A BBelum ada peringkat
- Mental Health Case StudyDokumen16 halamanMental Health Case Studyapi-472964417Belum ada peringkat
- RAHBAR NDMA-manual1 Compressed1Dokumen254 halamanRAHBAR NDMA-manual1 Compressed1SubhashiniBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- 2015 BH Service Manual PDFDokumen456 halaman2015 BH Service Manual PDFMike Andreini100% (1)
- 03.1 PHD Personality DisordersDokumen8 halaman03.1 PHD Personality DisordersDump AccBelum ada peringkat
- The Stockholm SyndromeDokumen2 halamanThe Stockholm SyndromeCatalina MihaelaBelum ada peringkat
- Parents WorkshopDokumen19 halamanParents WorkshopzakiBelum ada peringkat
- Schizoaffective With Bipolar DisordersDokumen14 halamanSchizoaffective With Bipolar DisordersNaomi MasudaBelum ada peringkat
- The Association Between Depression and Marital DissatisfactionDokumen22 halamanThe Association Between Depression and Marital DissatisfactionZuluaga LlanedBelum ada peringkat
- Discharge Plan 2.doc Imba - Doc123Dokumen4 halamanDischarge Plan 2.doc Imba - Doc123Hezron Ga33% (3)
- Mental Health Law Dissertation TopicsDokumen8 halamanMental Health Law Dissertation TopicsPayForSomeoneToWriteYourPaperUK100% (1)
- Social Motivation in ASD - Chevallier - Schultz - Presentation PDFDokumen10 halamanSocial Motivation in ASD - Chevallier - Schultz - Presentation PDFChrysoula Gkani100% (1)
- Positive Vs Negative ReinforcementDokumen3 halamanPositive Vs Negative ReinforcementHidayah Roslee100% (1)
- Psychosocial Correlates in Adolescent Children of Alcoholics-Implications For InterventionDokumen15 halamanPsychosocial Correlates in Adolescent Children of Alcoholics-Implications For InterventionYulinda AswanBelum ada peringkat
- Conduct Disorder in Children and Youth 1Dokumen11 halamanConduct Disorder in Children and Youth 1api-584579540Belum ada peringkat
- Employers' Perceptions and Attitudes Toward The Canadian National Standard On Psychological Health and Safety in The WorkplaceDokumen3 halamanEmployers' Perceptions and Attitudes Toward The Canadian National Standard On Psychological Health and Safety in The WorkplaceEgle UselieneBelum ada peringkat
- Psychology of Pregnant WomenDokumen27 halamanPsychology of Pregnant WomenAldrin ManuelBelum ada peringkat
- Health Optimizing Physical Education 1Dokumen22 halamanHealth Optimizing Physical Education 1Russel MejicoBelum ada peringkat
- NCD HandoutsDokumen7 halamanNCD HandoutsWilma Nierva BeraldeBelum ada peringkat
- Counselling and PsychoterapyDokumen52 halamanCounselling and PsychoterapyelnicaBelum ada peringkat