Anda mungkin juga menyukai
- Nursing the NeonateDari EverandNursing the NeonateMaggie MeeksBelum ada peringkat
- Neonatal SepsisDokumen51 halamanNeonatal SepsisAngelo Del VentoBelum ada peringkat
- Case Presentation On Neonatal Sepsis: BY-Anisha ManeDokumen45 halamanCase Presentation On Neonatal Sepsis: BY-Anisha ManeAnisha Mane100% (5)
- Neonatal SepsisDokumen53 halamanNeonatal SepsisFrancis AmuzuBelum ada peringkat
- Neonatal SepsisDokumen8 halamanNeonatal Sepsis+nellaBelum ada peringkat
- Φ PathophysiologyDokumen4 halamanΦ PathophysiologyMariah AshooriyanBelum ada peringkat
- Meconium Stained Amniotic FluidDokumen21 halamanMeconium Stained Amniotic FluidPoonam RanaBelum ada peringkat
- Neonatal SepsisDokumen5 halamanNeonatal SepsisBhawna PandhuBelum ada peringkat
- Neonatal Sepsis LectureDokumen142 halamanNeonatal Sepsis Lectureokwadha simion0% (1)
- Neonatal SepsisDokumen44 halamanNeonatal SepsisIsabel Barredo Del MundoBelum ada peringkat
- Meconium Aspiration Syndrome: Walter Otieno Consultant PaediatricianDokumen27 halamanMeconium Aspiration Syndrome: Walter Otieno Consultant PaediatricianMalueth AnguiBelum ada peringkat
- Necrotizing EnterocolitisDokumen24 halamanNecrotizing Enterocolitisfadhila khairunnisaBelum ada peringkat
- Neonatal SepsisDokumen29 halamanNeonatal SepsisElton Ndhlovu100% (3)
- Hellp SyndromeDokumen40 halamanHellp SyndromeChairunnisa Sitorus100% (2)
- MECONIUM Aspiration SyndromeDokumen37 halamanMECONIUM Aspiration SyndromekamalaBelum ada peringkat
- Respiratory Distress Syndrome in A Premature BabyDokumen29 halamanRespiratory Distress Syndrome in A Premature BabyVissalini JayabalanBelum ada peringkat
- PreeclampsiaDokumen14 halamanPreeclampsiaHenny NovitasariBelum ada peringkat
- Mechanism of LaborDokumen12 halamanMechanism of LaborSaidatul Safarah Md HassanBelum ada peringkat
- Ophthalmia NeonatorumDokumen19 halamanOphthalmia NeonatorumSanthu Tvm100% (1)
- NECDokumen32 halamanNECettevyviBelum ada peringkat
- Neonatal Hypoglycemia: 1.transient (Most Common) 2.persistenet (Less Common)Dokumen8 halamanNeonatal Hypoglycemia: 1.transient (Most Common) 2.persistenet (Less Common)mohammadBelum ada peringkat
- Neonatal PneumoniaDokumen16 halamanNeonatal Pneumoniaelyuchan100% (1)
- Seminar 6 Approach To Neonatal JaundiceDokumen50 halamanSeminar 6 Approach To Neonatal JaundiceKelvin Su100% (1)
- Meconium Aspiration SyndromeDokumen29 halamanMeconium Aspiration SyndromeAlwin Varghese T0% (1)
- Neonatal JaundiceDokumen30 halamanNeonatal JaundiceAnonymous Y3fqBduBelum ada peringkat
- Neonatal SepsisDokumen26 halamanNeonatal SepsisKimbek BuangkeBelum ada peringkat
- Asphyxia NeonatorumDokumen34 halamanAsphyxia NeonatorumListya Paramita100% (1)
- OLIGOHYDRAMNIOSDokumen3 halamanOLIGOHYDRAMNIOSRuzzel Cabrera-BermonteBelum ada peringkat
- Exchange Blood TransfusionDokumen38 halamanExchange Blood TransfusionMeseret Hamer Zewdie100% (1)
- Case Study Neonatal SepsisDokumen21 halamanCase Study Neonatal SepsisLenjun0% (1)
- Uterine Inversion1Dokumen26 halamanUterine Inversion1Meylinda OctavianaBelum ada peringkat
- Nephrotic SyndromeDokumen35 halamanNephrotic SyndromesudhaBelum ada peringkat
- Congenital Diaphragmatic HerniaDokumen21 halamanCongenital Diaphragmatic HerniaJennifer Dixon100% (1)
- Neonatal SepsisDokumen1 halamanNeonatal SepsisAnnsha VeimernBelum ada peringkat
- OB - II - PREGNANCY - HYPERTENSION - PDF Filename UTF-8''OB II PREGNANCY HYPERTENSIONDokumen10 halamanOB - II - PREGNANCY - HYPERTENSION - PDF Filename UTF-8''OB II PREGNANCY HYPERTENSIONyayayanizaBelum ada peringkat
- Meconium Aspiration: Ospital NG Maynila Medical Center Department of PediatricsDokumen38 halamanMeconium Aspiration: Ospital NG Maynila Medical Center Department of PediatricsGrace Antonette Pati100% (1)
- Neonatal JaundiceDokumen48 halamanNeonatal Jaundicelordoftheweb100% (22)
- Uremic Encephalopathy-ReviewDokumen30 halamanUremic Encephalopathy-ReviewFeddyFebriyantoManurung100% (1)
- Care of Unconscious PatientDokumen6 halamanCare of Unconscious PatientSuparna SinghaBelum ada peringkat
- Convulsive Disorders in ChildrenDokumen44 halamanConvulsive Disorders in ChildrenMurugesanBelum ada peringkat
- Case Study HELLPDokumen7 halamanCase Study HELLPJovirtBelum ada peringkat
- Hirschsprung DiseaseDokumen21 halamanHirschsprung DiseaseAhmad YaniBelum ada peringkat
- Congenital Anomalies in Newborn (Critical)Dokumen46 halamanCongenital Anomalies in Newborn (Critical)Shereen Mohamed Soliman HammoudaBelum ada peringkat
- Preventive Pediatrics Part 3Dokumen5 halamanPreventive Pediatrics Part 3mkct111Belum ada peringkat
- Meconium Aspiration SyndromeDokumen7 halamanMeconium Aspiration SyndromeAi Niech Inoel100% (1)
- Febrile SeizuresDokumen23 halamanFebrile SeizuresHafiz FadhliBelum ada peringkat
- Fetal DistressDokumen2 halamanFetal DistressBal Ri Mekoleu100% (1)
- Patent Ductus Arteriosus (PDA)Dokumen6 halamanPatent Ductus Arteriosus (PDA)Sintia MardhaBelum ada peringkat
- Poststreptococcal GlomerulonephritisDokumen19 halamanPoststreptococcal GlomerulonephritisAlex Ismael Catalan CabreraBelum ada peringkat
- Birth Asphyxia: by Anne E. Odaro MCM/2017/69852Dokumen26 halamanBirth Asphyxia: by Anne E. Odaro MCM/2017/69852ElvisBelum ada peringkat
- Inguinal Hernia: Shohreh Toutounchi Reference: Schwartz Principles of Surgery 2010 Internship: 1391Dokumen29 halamanInguinal Hernia: Shohreh Toutounchi Reference: Schwartz Principles of Surgery 2010 Internship: 1391Ritz CelsoBelum ada peringkat
- Hyperbilirubinemia of The Newborn-NicuDokumen4 halamanHyperbilirubinemia of The Newborn-NicuRamina HiponiaBelum ada peringkat
- Hypophosphat Emia: Presented By: Ramirez, Nichole Robles, Hannah Saquilayan, Kristine Siazon, ColeenDokumen37 halamanHypophosphat Emia: Presented By: Ramirez, Nichole Robles, Hannah Saquilayan, Kristine Siazon, ColeenKyle De Sagun OtedaBelum ada peringkat
- Risk Factors of Cesarean Delivery Due To Cephalopelvic Disproportion in Nulliparous Women at Sisaket HospitalDokumen7 halamanRisk Factors of Cesarean Delivery Due To Cephalopelvic Disproportion in Nulliparous Women at Sisaket HospitalManangioma ManBelum ada peringkat
- Neonatal NCPDokumen7 halamanNeonatal NCPMaria Delia SalvadoBelum ada peringkat
- Harika Priyanka. K Asst. Professor AconDokumen30 halamanHarika Priyanka. K Asst. Professor AconArchana MoreyBelum ada peringkat
- Premature Rupture of MembranesDokumen38 halamanPremature Rupture of MembranesArwa QishtaBelum ada peringkat
- PartographDokumen6 halamanPartographYep Yep100% (2)
- Angelic - Doc - Neonatal JaundiceDokumen16 halamanAngelic - Doc - Neonatal JaundiceAngy100% (5)
- Neonatal JaundiceDokumen33 halamanNeonatal JaundiceVaibhav Krishna100% (2)
- Jama Diaz 2021 LD 210051 1627992112.38089Dokumen3 halamanJama Diaz 2021 LD 210051 1627992112.38089Moe KebabBelum ada peringkat
- Jama Bates 2021 LD 210045 1626868722.2071Dokumen2 halamanJama Bates 2021 LD 210045 1626868722.2071Moe KebabBelum ada peringkat
- Biochemistry PDFDokumen47 halamanBiochemistry PDFMoe KebabBelum ada peringkat
- General Principles - AdditionsDokumen3 halamanGeneral Principles - AdditionsMoe KebabBelum ada peringkat
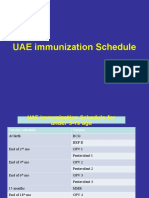
- Immunization Schedule UAEDokumen3 halamanImmunization Schedule UAEMoe KebabBelum ada peringkat
- Antiamoebic DrugsDokumen23 halamanAntiamoebic DrugsMoe KebabBelum ada peringkat
- Cestode SDokumen22 halamanCestode SMoe KebabBelum ada peringkat
- Mandibulofacial Dysostosis, Also Known As Treacher CollinsDokumen19 halamanMandibulofacial Dysostosis, Also Known As Treacher CollinsMoe KebabBelum ada peringkat
- T Collins SyndromeDokumen21 halamanT Collins SyndromeMoe KebabBelum ada peringkat
- Prognostic Factors Affecting The Mortality of Burn Injuries Patients in Dr. Sardjito General Hospital, Yogyakarta, IndonesiaDokumen8 halamanPrognostic Factors Affecting The Mortality of Burn Injuries Patients in Dr. Sardjito General Hospital, Yogyakarta, IndonesiaYeni PuspitasariBelum ada peringkat
- DRUG - STUDY CeferuximeDokumen6 halamanDRUG - STUDY Ceferuximepius troy macapazBelum ada peringkat
- Menstrupedia Comic: The Friendly Guide To Periods For Girls (2014), by Aditi Gupta, Tuhin Paul, and Rajat MittalDokumen4 halamanMenstrupedia Comic: The Friendly Guide To Periods For Girls (2014), by Aditi Gupta, Tuhin Paul, and Rajat MittalMy Home KaviBelum ada peringkat
- Janet RowleyDokumen1 halamanJanet RowleyANA GABRIELA PEREZ VIDALBelum ada peringkat
- Lab Report 15438869 20231127064225Dokumen1 halamanLab Report 15438869 20231127064225carilloabhe21Belum ada peringkat
- Iowa Neonatology HandbookDokumen11 halamanIowa Neonatology HandbookLowelly napitupuluBelum ada peringkat
- M.O.S DismantlingDokumen18 halamanM.O.S DismantlingAhmed Khaled100% (1)
- Tutorial Klinik: Widyarto Nugroho Pembimbing: Dr. M. Agung Pramudjito, SP - PDDokumen73 halamanTutorial Klinik: Widyarto Nugroho Pembimbing: Dr. M. Agung Pramudjito, SP - PDPutri PermataBelum ada peringkat
- 2014 09 - LOINC Tutorial - ImagingDokumen34 halaman2014 09 - LOINC Tutorial - ImagingDaniel VreemanBelum ada peringkat
- Etiology of Tuberculosis PDFDokumen2 halamanEtiology of Tuberculosis PDFKevinBelum ada peringkat
- Greene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Dokumen11 halamanGreene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Abigail HernándezBelum ada peringkat
- Reviewer RenalDokumen13 halamanReviewer Renalsean blaze100% (1)
- LIVER CHIRROSIS and GERED QUESTION AND ANSWERSDokumen10 halamanLIVER CHIRROSIS and GERED QUESTION AND ANSWERSjess_nookieBelum ada peringkat
- 03 NCP 5 Pulmonary Tuberculosis LalitDokumen17 halaman03 NCP 5 Pulmonary Tuberculosis Lalitamit100% (2)
- White Tongue Causes & 10 Natural Treatments For White Tongue - Dr. AxeDokumen10 halamanWhite Tongue Causes & 10 Natural Treatments For White Tongue - Dr. AxeRaghu100% (1)
- 3.2 Dr. Taufin SpOT - Operating RoomDokumen29 halaman3.2 Dr. Taufin SpOT - Operating RoomTaqwatin Ma'rifahBelum ada peringkat
- Care For Respiratory and Circulatory SystemsDokumen15 halamanCare For Respiratory and Circulatory SystemsJesse Kate GonzalesBelum ada peringkat
- Rashi - Effusion CytDokumen56 halamanRashi - Effusion CytShruthi N.RBelum ada peringkat
- Fenotipos Bioquímicos y Fagotipos de Cepas de Salmonella Enteritidis Aisladas en Antofagasta, 1997-2000Dokumen9 halamanFenotipos Bioquímicos y Fagotipos de Cepas de Salmonella Enteritidis Aisladas en Antofagasta, 1997-2000axel vargasBelum ada peringkat
- Livro Robbins PathologyDokumen18 halamanLivro Robbins Pathologyernestooliveira50% (2)
- Fadila Kemala Dwi Ramadhani Ruslan - Revisi Kbpji 2Dokumen16 halamanFadila Kemala Dwi Ramadhani Ruslan - Revisi Kbpji 2Eugenia RussiavBelum ada peringkat
- Presentation 1Dokumen36 halamanPresentation 1madhurima kunduBelum ada peringkat
- Joseph A. Ladapo, M.D., Ph.D. Curriculum Vitae Business InformationDokumen33 halamanJoseph A. Ladapo, M.D., Ph.D. Curriculum Vitae Business InformationWCTV Digital TeamBelum ada peringkat
- Test Bank ECGs Made Easy 5th Edition Barbara J AehlertDokumen10 halamanTest Bank ECGs Made Easy 5th Edition Barbara J AehlertErnest67% (3)
- HydrotherapyDokumen40 halamanHydrotherapyThopu UmamaheswariBelum ada peringkat
- Kantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Dokumen6 halamanKantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Ic-tika Siee ChuabbieBelum ada peringkat
- Arthrogryposis Multiplex Congenita-Dr S P DasDokumen7 halamanArthrogryposis Multiplex Congenita-Dr S P DasSheel GuptaBelum ada peringkat
- Patien Handout Hiv Aids During PregnancyDokumen3 halamanPatien Handout Hiv Aids During Pregnancyapi-317388058Belum ada peringkat
- Kenyaemr V17.3.1 Release Notes: Integration With Eid, Adt & Differential Upload DescriptionDokumen3 halamanKenyaemr V17.3.1 Release Notes: Integration With Eid, Adt & Differential Upload DescriptionMigori Art DataBelum ada peringkat