Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- 5 - Gastrointestinal Bleeding (AMBOSS) ?Dokumen6 halaman5 - Gastrointestinal Bleeding (AMBOSS) ?Rawabi rawabi1997Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- A Practical Guide To Obstetrics & Gynecology - Richa Saxena (2015) (PDF) (UnitedVRG) PDFDokumen506 halamanA Practical Guide To Obstetrics & Gynecology - Richa Saxena (2015) (PDF) (UnitedVRG) PDFPricope Elvis77% (13)
- The American Journal of Homoeopathy Vol. 3-4, 1849Dokumen362 halamanThe American Journal of Homoeopathy Vol. 3-4, 1849music75manBelum ada peringkat
- Mcqs in Medical Physiology 2014 EspDokumen138 halamanMcqs in Medical Physiology 2014 EspdaqBelum ada peringkat
- English For NursingDokumen30 halamanEnglish For NursingKiki SeptyantiBelum ada peringkat
- Puperal SepsisDokumen154 halamanPuperal SepsisOlal EmmaBelum ada peringkat
- Family Welfare Programme in IndiaDokumen25 halamanFamily Welfare Programme in IndiaTirumalesha DadigeBelum ada peringkat
- Flückinger's 1732 Report on the Meduegna Vampire OutbreakDokumen4 halamanFlückinger's 1732 Report on the Meduegna Vampire OutbreakLord Pindar100% (1)
- Women'S Health Deserves The Best: Philips Mammodiagnost DR Specifi CationDokumen12 halamanWomen'S Health Deserves The Best: Philips Mammodiagnost DR Specifi CationWilliam M. CamachoBelum ada peringkat
- 05 - DR - Dominicus - PELATIHAN DIFTERI TANGERANG 07 Jan 2018 - Tatalaksana - SharedDokumen48 halaman05 - DR - Dominicus - PELATIHAN DIFTERI TANGERANG 07 Jan 2018 - Tatalaksana - SharedArainy TikaBelum ada peringkat
- Jkms 32 974Dokumen11 halamanJkms 32 974KenBelum ada peringkat
- 7273935Dokumen12 halaman7273935KenBelum ada peringkat
- Meat IronDokumen33 halamanMeat IronKenBelum ada peringkat
- Anemia, Diet, and Therapeutic Iron Among Children Living With HIVDokumen9 halamanAnemia, Diet, and Therapeutic Iron Among Children Living With HIVKenBelum ada peringkat
- Anemia Malnutrition Molecular To Economic PathwaysDokumen39 halamanAnemia Malnutrition Molecular To Economic PathwaysKenBelum ada peringkat
- Indonesian Pediatric Endocrinology 4thDokumen14 halamanIndonesian Pediatric Endocrinology 4thGendis Ayu ArdiasBelum ada peringkat
- Risk factors for childhood lower respiratory infections in MongoliaDokumen7 halamanRisk factors for childhood lower respiratory infections in MongoliaKenBelum ada peringkat
- Total Serum Bilirubin Predicts Fat-Soluble Vitamin DeficiencyDokumen15 halamanTotal Serum Bilirubin Predicts Fat-Soluble Vitamin DeficiencyKenBelum ada peringkat
- Case Report: Staphylococcal Scalded Skin Syndrome in A NeonateDokumen7 halamanCase Report: Staphylococcal Scalded Skin Syndrome in A NeonateKenBelum ada peringkat
- Neonatal Parenteral Nutrition: Intensive Care Nursery House Staff ManualDokumen7 halamanNeonatal Parenteral Nutrition: Intensive Care Nursery House Staff ManualNugraha SultanBelum ada peringkat
- Evaluation of Leukocyte EsteraseDokumen5 halamanEvaluation of Leukocyte EsteraseKenBelum ada peringkat
- CCDokumen3 halamanCCKenBelum ada peringkat
- Anemia Dan Infection PDFDokumen3 halamanAnemia Dan Infection PDFKenBelum ada peringkat
- Evaluation of Cholestasis in Iranian Infants Less Than Three MonthsDokumen7 halamanEvaluation of Cholestasis in Iranian Infants Less Than Three MonthsKenBelum ada peringkat
- Beta AdrenergikDokumen9 halamanBeta AdrenergikKenBelum ada peringkat
- Aucity of Biliary DuctsDokumen10 halamanAucity of Biliary DuctsKenBelum ada peringkat
- Gejala Klinis Apa Sajakah Yang Bisa Digunakan UntukDokumen2 halamanGejala Klinis Apa Sajakah Yang Bisa Digunakan UntukKenBelum ada peringkat
- Korelasi Status Gizi, Asupan Zat Besi Dengan Feritin PDFDokumen8 halamanKorelasi Status Gizi, Asupan Zat Besi Dengan Feritin PDFKenBelum ada peringkat
- CC Prolong FeverDokumen3 halamanCC Prolong FeverKenBelum ada peringkat
- Lasia and Associated Pulmonary HypertensionDokumen12 halamanLasia and Associated Pulmonary HypertensionKenBelum ada peringkat
- Newborn Journal PDFDokumen8 halamanNewborn Journal PDFRose Ann ManalastasBelum ada peringkat
- Buttonhole DislocationDokumen13 halamanButtonhole DislocationHanif Andhika WardhanaBelum ada peringkat
- Discover The Positive Effects Prenatal Yoga: About The Holistic CenterDokumen2 halamanDiscover The Positive Effects Prenatal Yoga: About The Holistic CenterJerico RelopezBelum ada peringkat
- Maternal Sepsis 2022Dokumen13 halamanMaternal Sepsis 2022Erika RosasBelum ada peringkat
- Regional AnesthesiaDokumen33 halamanRegional Anesthesiashaq545Belum ada peringkat
- COGIParisAbstractBook 1Dokumen172 halamanCOGIParisAbstractBook 1Nawras AtassiBelum ada peringkat
- VIS Report FialDokumen16 halamanVIS Report FialAyaz MahmoodBelum ada peringkat
- Book ListDokumen3 halamanBook ListSolomon Seth SallforsBelum ada peringkat
- Enhanced Recovery ProtocolsDokumen17 halamanEnhanced Recovery ProtocolsHening Tirta KusumawardaniBelum ada peringkat
- Tintinalli - Chapter 37 Procedural Sedation and Analgesia in AdultsDokumen11 halamanTintinalli - Chapter 37 Procedural Sedation and Analgesia in AdultsPgmee KimsBelum ada peringkat
- Multiple Choice Questions For Urinary Obstruction and BPH: E. Too Much Urine Produced by The KidneyDokumen3 halamanMultiple Choice Questions For Urinary Obstruction and BPH: E. Too Much Urine Produced by The KidneyOe MahardikaBelum ada peringkat
- Introduction To Endocrinology For Clinical StudentsDokumen9 halamanIntroduction To Endocrinology For Clinical StudentsOhwovoriole ToketemuBelum ada peringkat
- Nursing Theory Development BulletsDokumen2 halamanNursing Theory Development Bulletstorque1583% (6)
- Pelvic Inflammatory DiseaseDokumen3 halamanPelvic Inflammatory DiseaseRania S. HamdanBelum ada peringkat
- Clinical TeachingDokumen21 halamanClinical Teachingtanmai nooluBelum ada peringkat
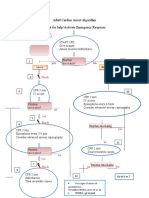
- Adult Cardiac Arrest Treatment AlgorithmDokumen1 halamanAdult Cardiac Arrest Treatment AlgorithmICU RSBMBelum ada peringkat
- Consolidated List of Casualties Treated in InfirmaryDokumen9 halamanConsolidated List of Casualties Treated in Infirmaryapi-293976957Belum ada peringkat
- Pacemaker Physics PaperDokumen7 halamanPacemaker Physics PaperJose Rene BerliozBelum ada peringkat
- Jurnal - Comparative Study of Male and Female Sebum Production 2017Dokumen6 halamanJurnal - Comparative Study of Male and Female Sebum Production 2017Melvy RozaBelum ada peringkat
- Guidelines for Starting X-Ray InstallationDokumen3 halamanGuidelines for Starting X-Ray InstallationmansooracBelum ada peringkat
- Total Hip Replacement Recovery & Surgery Complications - Dr. Vinil ShindeDokumen2 halamanTotal Hip Replacement Recovery & Surgery Complications - Dr. Vinil ShindeDr VInil ShindeBelum ada peringkat