Anda mungkin juga menyukai
- Microbio Lab 6Dokumen4 halamanMicrobio Lab 6api-374321750% (2)
- Nematodes and Cestodes OutlineDokumen6 halamanNematodes and Cestodes OutlineFarlogy80% (5)
- Parasitology HandoutsDokumen12 halamanParasitology HandoutsJed Imperial100% (1)
- CestodesDokumen4 halamanCestodesmrcveight100% (1)
- Clin Path Lab 6 UrinalysisDokumen5 halamanClin Path Lab 6 Urinalysisapi-3743217100% (6)
- ParasitologyDokumen27 halamanParasitologyDreyden HaloBelum ada peringkat
- Parasitology Table ReviewDokumen8 halamanParasitology Table ReviewAliehsEiram18Belum ada peringkat
- WWW - Ib.academy: Study GuideDokumen122 halamanWWW - Ib.academy: Study GuideHendrikEspinozaLoyola100% (2)
- Cestodes (Table)Dokumen3 halamanCestodes (Table)Marelle M. Yamzon87% (15)
- Parasitology TableDokumen4 halamanParasitology TableJae MinionBelum ada peringkat
- Parasitology TablesDokumen9 halamanParasitology Tables2013SecB92% (25)
- Microbiology (Bacteriolog) Lab - Practicals 1Dokumen4 halamanMicrobiology (Bacteriolog) Lab - Practicals 1Junno Turiano95% (20)
- Intestinal Nematodes (Unholy Trinity)Dokumen6 halamanIntestinal Nematodes (Unholy Trinity)DAN JR. M. BAUSABelum ada peringkat
- Microbio Lab 7 (Leigh)Dokumen8 halamanMicrobio Lab 7 (Leigh)api-3743217100% (6)
- Para Lab 2Dokumen3 halamanPara Lab 2api-3743217100% (2)
- Quarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The PhilippinesDokumen21 halamanQuarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The Philippinestricia100% (5)
- Virology TableDokumen10 halamanVirology TablekevinBelum ada peringkat
- Parasitology-Lec 10 EntamoebaDokumen7 halamanParasitology-Lec 10 Entamoebaapi-3743217100% (2)
- Microbio Lec 5 - StaphylococcusDokumen6 halamanMicrobio Lec 5 - Staphylococcusapi-3743217100% (2)
- Parasitology Lec ReviewerDokumen10 halamanParasitology Lec ReviewerPatricia Ann JoseBelum ada peringkat
- Parasitology Reviewer: Monica Kristine ReyesDokumen34 halamanParasitology Reviewer: Monica Kristine ReyesMariel Yanes Garcia75% (4)
- Clinical Parasitology Lecture NotesDokumen14 halamanClinical Parasitology Lecture NotesWei Zel Bolongon100% (2)
- Parasitology (Laboratory) - Trichuris TrichiuraDokumen4 halamanParasitology (Laboratory) - Trichuris TrichiuraJunno Turiano100% (1)
- RA 9344 As Amended by RA 10630 - HandoutsDokumen9 halamanRA 9344 As Amended by RA 10630 - HandoutsJan Re Espina CadeleñaBelum ada peringkat
- Filipino HousesDokumen4 halamanFilipino HousesjackBelum ada peringkat
- ParasitologyDokumen15 halamanParasitologyamelia_ericaBelum ada peringkat
- Microbio Lec 8 - MycobacteriaDokumen6 halamanMicrobio Lec 8 - Mycobacteriaapi-374321750% (2)
- Parasitology-Lec 13 MalariaDokumen6 halamanParasitology-Lec 13 Malariaapi-3743217Belum ada peringkat
- TREMATODESDokumen10 halamanTREMATODESAngel Pico100% (4)
- TREMATODESDokumen3 halamanTREMATODESMeccar Moniem H. Elino100% (6)
- Microbio Lab 8Dokumen4 halamanMicrobio Lab 8api-3743217100% (5)
- Microbio Lab 8Dokumen4 halamanMicrobio Lab 8api-3743217100% (5)
- Clinical Bacteriology ReviewerDokumen17 halamanClinical Bacteriology Reviewernkivc100% (5)
- Protozoa Summary TableDokumen1 halamanProtozoa Summary TablejustBelum ada peringkat
- Nematodes For Quiz 1 RevisedDokumen6 halamanNematodes For Quiz 1 RevisedAra NuesaBelum ada peringkat
- Medical Parasitology in Tables PDFDokumen15 halamanMedical Parasitology in Tables PDFRami Mohammed86% (7)
- Para Lab 1Dokumen3 halamanPara Lab 1api-3743217100% (1)
- Practical Manual for Detection of Parasites in Feces, Blood and Urine SamplesDari EverandPractical Manual for Detection of Parasites in Feces, Blood and Urine SamplesBelum ada peringkat
- s4 l3 Nematodes IIDokumen14 halamans4 l3 Nematodes II2013SecB100% (1)
- Clin Path Lab 6 Urinalysis Part 2Dokumen7 halamanClin Path Lab 6 Urinalysis Part 2api-3743217100% (3)
- Mtap Batch 2 MidtermsDokumen75 halamanMtap Batch 2 MidtermsLea JuanBelum ada peringkat
- s4 l2 Nematodes IDokumen8 halamans4 l2 Nematodes I2013SecBBelum ada peringkat
- Parasitology Table: ProtozoaDokumen10 halamanParasitology Table: ProtozoaKate Alyssa CatonBelum ada peringkat
- Parasitology-Lec 6 Liver Flukes (Kat)Dokumen7 halamanParasitology-Lec 6 Liver Flukes (Kat)api-3743217100% (1)
- Parasitology-Lec 5 TrematodesDokumen5 halamanParasitology-Lec 5 Trematodesapi-3743217100% (2)
- Microbio Lec 5 - StreptococcusDokumen6 halamanMicrobio Lec 5 - Streptococcusapi-3743217100% (4)
- NematodesDokumen2 halamanNematodesNicole TanBelum ada peringkat
- MycologyDokumen26 halamanMycologySkandi43Belum ada peringkat
- Protozoa RevisionDokumen6 halamanProtozoa Revisionfiena92100% (1)
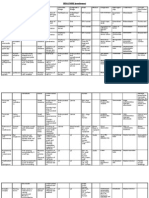
- Parasite Common Name Disease Is and Ds Morphology Lab Diagnosis Pathology Epidemiol OGY TreatmentDokumen2 halamanParasite Common Name Disease Is and Ds Morphology Lab Diagnosis Pathology Epidemiol OGY TreatmentMartin Clyde100% (5)
- Lecture Notes - MEDICAL PARASITOLOGYDokumen12 halamanLecture Notes - MEDICAL PARASITOLOGYAngelica Marzo67% (3)
- Parasitology-Lec 3 Nematodes 2Dokumen6 halamanParasitology-Lec 3 Nematodes 2api-3743217100% (4)
- Microbio Lec 10 - Enterobacteriaceae Gen, Shigella and SalmoDokumen8 halamanMicrobio Lec 10 - Enterobacteriaceae Gen, Shigella and Salmoapi-3743217100% (7)
- Creating Literacy Instruction For All Students ResourceDokumen25 halamanCreating Literacy Instruction For All Students ResourceNicole RickettsBelum ada peringkat
- Clin Path Lab 3Dokumen3 halamanClin Path Lab 3api-3743217100% (1)
- Parasitology Lec 3.01b Blood and Tissue NematodesDokumen15 halamanParasitology Lec 3.01b Blood and Tissue NematodesEnaWahahaBelum ada peringkat
- Parasitology-Lec 7 Lung FlukesDokumen5 halamanParasitology-Lec 7 Lung Flukesapi-3743217100% (1)
- Parasitology-Lec 9 CestodesDokumen5 halamanParasitology-Lec 9 Cestodesapi-3743217100% (4)
- Microbio Lec 2 - Physio of Bacterial GrowthDokumen4 halamanMicrobio Lec 2 - Physio of Bacterial Growthapi-37432170% (1)
- NematodesDokumen10 halamanNematodesNicolette Go100% (1)
- Microbio Lec 4 - Microbial Flora in Health and DiseaseDokumen2 halamanMicrobio Lec 4 - Microbial Flora in Health and Diseaseapi-374321750% (2)
- Parasitology-Lec 12 TrypanosomesDokumen6 halamanParasitology-Lec 12 Trypanosomesapi-3743217Belum ada peringkat
- CestodesDokumen10 halamanCestodessarguss14100% (1)
- Parasitology (Laboratory) - NEMATODES - Ascaris LumbricoidesDokumen9 halamanParasitology (Laboratory) - NEMATODES - Ascaris LumbricoidesJunno Turiano100% (2)
- Helminth 5Dokumen5 halamanHelminth 5fiena92100% (2)
- Para Lab 8Dokumen2 halamanPara Lab 8api-3743217100% (2)
- PROTOZOAN Part 2Dokumen1 halamanPROTOZOAN Part 2Meccar Moniem H. ElinoBelum ada peringkat
- 2 PARA 1 - Protozoa - FlagellatesDokumen13 halaman2 PARA 1 - Protozoa - FlagellatesTricia LlorinBelum ada peringkat
- BELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Dokumen69 halamanBELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Sharon Agor0% (1)
- Medical Biology 6Dokumen58 halamanMedical Biology 6Yusuf Yağız TimurBelum ada peringkat
- Veterinary Helminthology MidtermsDokumen4 halamanVeterinary Helminthology Midtermshumanupgrade100% (1)
- STH's Unholy TrinityDokumen8 halamanSTH's Unholy TrinityEunice AndradeBelum ada peringkat
- STH's Unholy TrinityDokumen9 halamanSTH's Unholy TrinityEunice AndradeBelum ada peringkat
- Clin Path Lab 7Dokumen1 halamanClin Path Lab 7api-3743217Belum ada peringkat
- Microbio Lec 12 - Treponema Borrelia, Helicobacter LegioneDokumen6 halamanMicrobio Lec 12 - Treponema Borrelia, Helicobacter Legioneapi-374321750% (2)
- Microbio Lec 13 - Ricketssiacea Chlamydiae, MycoplasmaDokumen3 halamanMicrobio Lec 13 - Ricketssiacea Chlamydiae, Mycoplasmaapi-3743217Belum ada peringkat
- Microbio Lec 11 - Ecoli, Klebsiella Proteus, Citrobacter AnDokumen3 halamanMicrobio Lec 11 - Ecoli, Klebsiella Proteus, Citrobacter Anapi-374321750% (2)
- Clin Path Lec 1 - GeneralitiesDokumen3 halamanClin Path Lec 1 - Generalitiesapi-3743217Belum ada peringkat
- Microbio Lec 8 - Bacteroides Actinomyces PropionibacteriumDokumen3 halamanMicrobio Lec 8 - Bacteroides Actinomyces Propionibacteriumapi-37432170% (1)
- Microbio Lec 9 - Hemophilus Bordetella Francis Ella, BrucelDokumen5 halamanMicrobio Lec 9 - Hemophilus Bordetella Francis Ella, Brucelapi-37432170% (1)
- Microbio Lab 9,10,11,12 & ReviewDokumen3 halamanMicrobio Lab 9,10,11,12 & Reviewapi-374321750% (2)
- Microbio Lec 7 - Clostridium and BacillusDokumen5 halamanMicrobio Lec 7 - Clostridium and Bacillusapi-3743217100% (1)
- Microbio Lab 4Dokumen3 halamanMicrobio Lab 4api-3743217100% (2)
- Pa Tho Genesis of Bacterial InfectionDokumen5 halamanPa Tho Genesis of Bacterial Infectionapi-374321750% (2)
- Microbio Lab 5Dokumen2 halamanMicrobio Lab 5api-37432170% (1)
- Microbio Lec 6 - Strep PneumoniaeDokumen2 halamanMicrobio Lec 6 - Strep Pneumoniaeapi-3743217Belum ada peringkat
- Microbio Lec 6 - NeisseriaDokumen3 halamanMicrobio Lec 6 - Neisseriaapi-3743217Belum ada peringkat
- Microbio Lec 3 - Sterilization and DisinfectionDokumen3 halamanMicrobio Lec 3 - Sterilization and Disinfectionapi-3743217Belum ada peringkat
- Microbio Lec 4 - Host-Parasite RelationshipDokumen2 halamanMicrobio Lec 4 - Host-Parasite Relationshipapi-3743217100% (1)
- Microbio Lec 1 - Bacterial Morphology and Ultra StructureDokumen8 halamanMicrobio Lec 1 - Bacterial Morphology and Ultra Structureapi-3743217100% (3)
- Microbio Lab 1 and 2 U 2006Dokumen6 halamanMicrobio Lab 1 and 2 U 2006api-3743217100% (2)
- Forecast Error (Control Chart)Dokumen2 halamanForecast Error (Control Chart)Jane OngBelum ada peringkat
- Olinger v. The Church of Jesus Christ of Latter Day Saints Et Al - Document No. 1Dokumen4 halamanOlinger v. The Church of Jesus Christ of Latter Day Saints Et Al - Document No. 1Justia.comBelum ada peringkat
- Commercial CrimesDokumen3 halamanCommercial CrimesHo Wen HuiBelum ada peringkat
- Lecture 6Dokumen7 halamanLecture 6Shuja MirBelum ada peringkat
- Final Research ReportDokumen14 halamanFinal Research ReportAlojado Lamuel Jesu ABelum ada peringkat
- The Role of Personalization, Engagement and Trust in Online CommunitiesDokumen17 halamanThe Role of Personalization, Engagement and Trust in Online CommunitiesAbiBelum ada peringkat
- 15 Melodic Uses of Non-Chord TonesDokumen3 halaman15 Melodic Uses of Non-Chord TonesonlymusicaBelum ada peringkat
- Debus Medical RenaissanceDokumen3 halamanDebus Medical RenaissanceMarijaBelum ada peringkat
- BIO210 Lab Report 3Dokumen6 halamanBIO210 Lab Report 3Isra MallaBelum ada peringkat
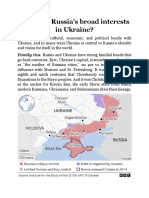
- What Are RussiaDokumen3 halamanWhat Are RussiaMuhammad SufyanBelum ada peringkat
- Arsu and AzizoDokumen123 halamanArsu and AzizoZebu BlackBelum ada peringkat
- GST 101 Exam Past QuestionsDokumen6 halamanGST 101 Exam Past QuestionsBenjamin Favour100% (2)
- Rape and Challenging Contemporary ThinkingDokumen17 halamanRape and Challenging Contemporary ThinkingKirthna MadhavanBelum ada peringkat
- Analysis of Low-Frequency Passive Seismic Attributes in Maroun Oil Field, IranDokumen16 halamanAnalysis of Low-Frequency Passive Seismic Attributes in Maroun Oil Field, IranFakhrur NoviantoBelum ada peringkat
- Engineering Road Note 9 - May 2012 - Uploaded To Main Roads Web SiteDokumen52 halamanEngineering Road Note 9 - May 2012 - Uploaded To Main Roads Web SiteRahma SariBelum ada peringkat
- Measures-English, Metric, and Equivalents PDFDokumen1 halamanMeasures-English, Metric, and Equivalents PDFluz adolfoBelum ada peringkat
- Aìgas of Bhakti. at The End of The Last Chapter Uddhava Inquired AboutDokumen28 halamanAìgas of Bhakti. at The End of The Last Chapter Uddhava Inquired AboutDāmodar DasBelum ada peringkat
- 2022BusinessManagement ReportDokumen17 halaman2022BusinessManagement ReportkianaBelum ada peringkat
- Fascinating Numbers: Some Numbers of 3 Digits or More Exhibit A Very Interesting PropertyDokumen2 halamanFascinating Numbers: Some Numbers of 3 Digits or More Exhibit A Very Interesting PropertyAnonymous JGW0KRl6Belum ada peringkat
- Implementation of 7s Framenwork On RestuDokumen36 halamanImplementation of 7s Framenwork On RestuMuhammad AtaBelum ada peringkat
- 1sebastian Vs CalisDokumen6 halaman1sebastian Vs CalisRai-chan Junior ÜBelum ada peringkat
- English Lesson PlanDokumen3 halamanEnglish Lesson PlanJeremias MartirezBelum ada peringkat
- Sri Guru Parampara Stotram CompressDokumen14 halamanSri Guru Parampara Stotram CompressSatishPavurayalaBelum ada peringkat
- COMM 103 Floyd Chapters Study GuideDokumen4 halamanCOMM 103 Floyd Chapters Study GuideMad BasblaBelum ada peringkat
- Symbiosis National Aptitude Test (SNAP) 2004: InstructionsDokumen21 halamanSymbiosis National Aptitude Test (SNAP) 2004: InstructionsHarsh JainBelum ada peringkat