Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Credit Card StatementDokumen4 halamanCredit Card StatementHe HdhdjBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Account Statement CapitecDokumen4 halamanAccount Statement CapitecVince Smart100% (1)
- JennylynreductocleofeDokumen4 halamanJennylynreductocleofeLia Estrelle CleofeBelum ada peringkat
- Innovation and PrivacyDokumen11 halamanInnovation and PrivacyEddy D. SánchezBelum ada peringkat
- Easy eBay carding method for items up to $600Dokumen4 halamanEasy eBay carding method for items up to $600Mendel AssouanBelum ada peringkat
- 2019 April StatementDokumen2 halaman2019 April Statementkumar samyappanBelum ada peringkat
- AXIS BANK Statement For April 2019Dokumen2 halamanAXIS BANK Statement For April 2019Innovacion Airconditioning100% (1)
- Petty Cash VoucherDokumen4 halamanPetty Cash VoucherUgen SparkBelum ada peringkat
- The Indian Payments Handbook 2021 2026Dokumen34 halamanThe Indian Payments Handbook 2021 2026scienceplexBelum ada peringkat
- Joint Resolution To Put Non-Partisan Redistricting Before WI VotersDokumen1 halamanJoint Resolution To Put Non-Partisan Redistricting Before WI VotersCommonCauseWIBelum ada peringkat
- 2013-2014 Non-Partisan Redistricting Reform in WisconsinDokumen3 halaman2013-2014 Non-Partisan Redistricting Reform in WisconsinCommonCauseWIBelum ada peringkat
- WI Senate Bill 148 (Page 7)Dokumen1 halamanWI Senate Bill 148 (Page 7)CommonCauseWIBelum ada peringkat
- Judge Strikes Down WI Voter ID Law - 4!29!2014Dokumen2 halamanJudge Strikes Down WI Voter ID Law - 4!29!2014CommonCauseWIBelum ada peringkat
- Common Cause in WI Dec 3, 2013 Press Release - "Many Less Competitive State Legislative and Congressional Elections"Dokumen2 halamanCommon Cause in WI Dec 3, 2013 Press Release - "Many Less Competitive State Legislative and Congressional Elections"CommonCauseWIBelum ada peringkat
- Kenosha News Editorial On Redistricting Reform - September 14, 2013Dokumen1 halamanKenosha News Editorial On Redistricting Reform - September 14, 2013CommonCauseWIBelum ada peringkat
- WI Redistricting Reform Co-Sponsors As of 9-30-2013Dokumen1 halamanWI Redistricting Reform Co-Sponsors As of 9-30-2013CommonCauseWIBelum ada peringkat
- Amici Curiae in The Case of Jones v. DeiningerDokumen19 halamanAmici Curiae in The Case of Jones v. DeiningerCommonCauseWIBelum ada peringkat
- WI Redistricting Reform Co-Sponsors - As of 9-17-2013Dokumen1 halamanWI Redistricting Reform Co-Sponsors - As of 9-17-2013CommonCauseWIBelum ada peringkat
- Home News Article - 11-16-2011Dokumen2 halamanHome News Article - 11-16-2011CommonCauseWIBelum ada peringkat
- WI Congressional Fundraising Totals 2012Dokumen4 halamanWI Congressional Fundraising Totals 2012CommonCauseWIBelum ada peringkat
- CCWI October 23rd Press ReleaseDokumen1 halamanCCWI October 23rd Press ReleaseCommonCauseWIBelum ada peringkat
- Toxic Spending Wisconsin Release Version 2.pagesDokumen2 halamanToxic Spending Wisconsin Release Version 2.pagesCommonCauseWIBelum ada peringkat
- Amici Curiae in The Case of Jones v. DeiningerDokumen19 halamanAmici Curiae in The Case of Jones v. DeiningerCommonCauseWIBelum ada peringkat
- Contribution FormDokumen1 halamanContribution FormCommonCauseWIBelum ada peringkat
- Common Cause ALEC Release For 8-4-11Dokumen2 halamanCommon Cause ALEC Release For 8-4-11CommonCauseWIBelum ada peringkat
- Committees and Boards For Which The Wisconsin Supreme Court Seeks Lawyer and Non-Lawyer ApplicantsDokumen3 halamanCommittees and Boards For Which The Wisconsin Supreme Court Seeks Lawyer and Non-Lawyer ApplicantsCommonCauseWIBelum ada peringkat
- Renewed Motion To InterveneDokumen20 halamanRenewed Motion To InterveneCommonCauseWIBelum ada peringkat
- Plaintiff's Motion Restraining Order Injunction - 764 (00549210)Dokumen4 halamanPlaintiff's Motion Restraining Order Injunction - 764 (00549210)CommonCauseWIBelum ada peringkat
- Former Wisconsin Legislator Cal Potter To Join CCWI BoardDokumen2 halamanFormer Wisconsin Legislator Cal Potter To Join CCWI BoardCommonCauseWIBelum ada peringkat
- Proposed EmR Order 1 28Dokumen7 halamanProposed EmR Order 1 28CommonCauseWIBelum ada peringkat
- KSA IFCR - G20 Edition - 24 Nov 2020 - B6cespDokumen172 halamanKSA IFCR - G20 Edition - 24 Nov 2020 - B6cespFina AlfiahBelum ada peringkat
- Pulse of Fintech 2018: Blockchain Investment Exceeds 2017 Annual TotalDokumen2 halamanPulse of Fintech 2018: Blockchain Investment Exceeds 2017 Annual TotalSergio VinsennauBelum ada peringkat
- Customer's Perception Towards Digital WalletDokumen5 halamanCustomer's Perception Towards Digital WalletWynona PinlacBelum ada peringkat
- SRS Document - Project ArrowDokumen4 halamanSRS Document - Project ArrowRanier RanierBelum ada peringkat
- Statement of AccountDokumen6 halamanStatement of AccountVikasBelum ada peringkat
- OrderForm Pipeline-Forecaster VNDokumen1 halamanOrderForm Pipeline-Forecaster VNshengchanBelum ada peringkat
- Dec 2021. VattamDokumen11 halamanDec 2021. VattamsadaSivaBelum ada peringkat
- Statement 2023 8Dokumen1 halamanStatement 2023 89jhdh8qthtBelum ada peringkat
- TNG Ewallet TransactionsDokumen73 halamanTNG Ewallet TransactionsaBelum ada peringkat
- Warranty Card #BML9726Dokumen1 halamanWarranty Card #BML9726tanBelum ada peringkat
- How The M Pesa WorksDokumen2 halamanHow The M Pesa WorksBrianBelum ada peringkat
- Account Statement 011118 011218 PDFDokumen8 halamanAccount Statement 011118 011218 PDFSwarupBelum ada peringkat
- 14410628-Ta-Muhammad Ilham Agus Salim-Legal Protection For User Data in Fintech Peer To Peer Lending Rupiah CepatDokumen115 halaman14410628-Ta-Muhammad Ilham Agus Salim-Legal Protection For User Data in Fintech Peer To Peer Lending Rupiah CepatHam AgsaBelum ada peringkat
- Buy Bitcoin Instantly Paxful 11Dokumen1 halamanBuy Bitcoin Instantly Paxful 11Richie DcBelum ada peringkat
- AccountStatement28-10-2023 To 31-03-2024Dokumen39 halamanAccountStatement28-10-2023 To 31-03-2024humanresourcesphoenixassuranceBelum ada peringkat
- e-StatementBRImo 422901012590530 Dec2023 20231226 173853Dokumen3 halamane-StatementBRImo 422901012590530 Dec2023 20231226 173853abieyandrasusantoBelum ada peringkat
- 1579603422694Dokumen10 halaman1579603422694Nazeer HussainBelum ada peringkat
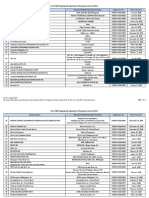
- List of BSP Registered Operator of Payment System (OPS)Dokumen11 halamanList of BSP Registered Operator of Payment System (OPS)Don Jose ReclamadoBelum ada peringkat
- Tigo Pesa Account StatementDokumen7 halamanTigo Pesa Account StatementPeter Ngicur Carthemi100% (1)
- EpaymentDokumen6 halamanEpaymentvyknk21Belum ada peringkat
- Account Statement For The Account: 3127000108458731: Branch DetailsDokumen8 halamanAccount Statement For The Account: 3127000108458731: Branch DetailsDEVENDRA KUMAR SHEETAL0% (1)