Anda mungkin juga menyukai
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDari EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideBelum ada peringkat
- Hydatidiform Mole Diagnosis and ManagementDokumen19 halamanHydatidiform Mole Diagnosis and ManagementAndre Karl FaculinBelum ada peringkat
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- STIs 2Dokumen15 halamanSTIs 2cfarley04Belum ada peringkat
- Sti RtiDokumen88 halamanSti RtiDr.L.R.Ahirwar100% (1)
- Chronic Kidney FailureDokumen9 halamanChronic Kidney FailureKrizzy MontanaBelum ada peringkat
- The Primary Goal of MCNDokumen12 halamanThe Primary Goal of MCNAira Marie DoroteoBelum ada peringkat
- Abuse and Violence: Abuse Is The Wrongful Use and Maltreatment of Another PersonDokumen10 halamanAbuse and Violence: Abuse Is The Wrongful Use and Maltreatment of Another PersonjacnpoyBelum ada peringkat
- AmebiasisDokumen14 halamanAmebiasisxxxchi chaxxxBelum ada peringkat
- Mouth Care To Reduce Ventilator Associated.22Dokumen7 halamanMouth Care To Reduce Ventilator Associated.22heartbcglBelum ada peringkat
- Primary Health Care Maternal & Child HealthDokumen32 halamanPrimary Health Care Maternal & Child HealthAbidah Rahmi HilmyBelum ada peringkat
- Sexually Transmitted InfectionsDokumen16 halamanSexually Transmitted InfectionsNatukunda DianahBelum ada peringkat
- CHN Health PromotionDokumen7 halamanCHN Health PromotionNareeza AbdullaBelum ada peringkat
- Health Promotion and Disease PreventionDokumen32 halamanHealth Promotion and Disease PreventionThibahar RajendranBelum ada peringkat
- Postpartum Physical and Emotional Assessment GuideDokumen39 halamanPostpartum Physical and Emotional Assessment GuidePerrilyn PereyBelum ada peringkat
- Lemone 6e Chapter 31Dokumen47 halamanLemone 6e Chapter 31Husein Fatih ArafatBelum ada peringkat
- Hiv in PregnancyDokumen13 halamanHiv in Pregnancyapi-533578725Belum ada peringkat
- Nursing Concept Map 1Dokumen3 halamanNursing Concept Map 1Norah Okafor Ezike67% (3)
- Urinary Tract Infection (UTI) : A Guide For WomenDokumen2 halamanUrinary Tract Infection (UTI) : A Guide For WomenBily ManBelum ada peringkat
- Hypervolemia What You Need To Know About Fluid OverloadDokumen3 halamanHypervolemia What You Need To Know About Fluid OverloadLorenn AdarnaBelum ada peringkat
- Ch34 PharmDokumen8 halamanCh34 PharmShaneka WilliamsBelum ada peringkat
- Mental Health RemediationDokumen3 halamanMental Health RemediationAlvin L. Rozier100% (2)
- Managing Anger, Hostility and AggressionDokumen11 halamanManaging Anger, Hostility and AggressionNoha DimapunongBelum ada peringkat
- WEEK 1 - Concept of CommunityDokumen5 halamanWEEK 1 - Concept of Communitypoleene de leonBelum ada peringkat
- Reflective EssayDokumen2 halamanReflective EssayAnonymous 0CdrZVBelum ada peringkat
- Care PlanDokumen26 halamanCare PlanChevelle Valenciano-GaanBelum ada peringkat
- Thyroid StormDokumen15 halamanThyroid Stormdr_arvindanBelum ada peringkat
- Critical Thinking Case Study PharmaDokumen2 halamanCritical Thinking Case Study Pharmakimberly magsipocBelum ada peringkat
- Sexually Transmitted InfectionsDokumen34 halamanSexually Transmitted InfectionsMariana Creciun100% (1)
- Filipino Family Dynamics and Cultural Health PracticesDokumen6 halamanFilipino Family Dynamics and Cultural Health Practicesanette katrinBelum ada peringkat
- Nursing Bullets: Fundamentals of Nursing ReviewerDokumen44 halamanNursing Bullets: Fundamentals of Nursing ReviewerErl DiamanteBelum ada peringkat
- Phar 185 Global Health UpdatesDokumen7 halamanPhar 185 Global Health UpdatesKristel Keith NievaBelum ada peringkat
- MARCOS - Legal Issues of ElderlyDokumen2 halamanMARCOS - Legal Issues of ElderlyArian May MarcosBelum ada peringkat
- Fluid Electrolytes and Acid Base BalanceDokumen108 halamanFluid Electrolytes and Acid Base BalancesayednourBelum ada peringkat
- Health Education PlanDokumen10 halamanHealth Education PlanJulienne Sanchez-SalazarBelum ada peringkat
- Capstone Paper Summative FINAL VERSIONDokumen10 halamanCapstone Paper Summative FINAL VERSIONoliviajuolaBelum ada peringkat
- Heart and Neck VesselsDokumen3 halamanHeart and Neck VesselsMark ElbenBelum ada peringkat
- NCM 120 TOPIC 1-3 Cultural Health Assessment ModelsDokumen7 halamanNCM 120 TOPIC 1-3 Cultural Health Assessment ModelsGhianx Carlox PioquintoxBelum ada peringkat
- Principles of Health EducationDokumen7 halamanPrinciples of Health EducationSonu SubbaBelum ada peringkat
- Admintrationofmedications1 Copy 181202173921Dokumen186 halamanAdmintrationofmedications1 Copy 181202173921Karl RobleBelum ada peringkat
- Primary HealthcareDokumen5 halamanPrimary HealthcareCHELSEA MOLINOS JUANBelum ada peringkat
- INTRODUCTION TO GLOBAL HEALTH LessonsDokumen39 halamanINTRODUCTION TO GLOBAL HEALTH LessonsDeidra Borus100% (1)
- ETOH Case StudyDokumen5 halamanETOH Case StudyCharme Jean RaygonBelum ada peringkat
- Hyperthyroidism GuideDokumen40 halamanHyperthyroidism GuidemypublicidBelum ada peringkat
- Hyperthyroidism Causes, Symptoms, Diagnosis and TreatmentDokumen40 halamanHyperthyroidism Causes, Symptoms, Diagnosis and TreatmentEmmanuelBelum ada peringkat
- The Infant Should Always Be in A Rear-Facing Car Seat From Birth To 9.1 KGDokumen7 halamanThe Infant Should Always Be in A Rear-Facing Car Seat From Birth To 9.1 KGSabhi Sandhu100% (1)
- Health Promotion Plan for COVID-19 VaccinationsDokumen5 halamanHealth Promotion Plan for COVID-19 VaccinationsGeorge KavuviBelum ada peringkat
- HIV Treatment 2Dokumen3 halamanHIV Treatment 2kimglaidyl bontuyanBelum ada peringkat
- Withdrawal (Coitus Interruptus)Dokumen9 halamanWithdrawal (Coitus Interruptus)Mochammad Adam EldiBelum ada peringkat
- Pediatric NursingDokumen4 halamanPediatric Nursingjustjesko0lBelum ada peringkat
- INFECTION CONTROL: CAN NURSES IMPROVE HAND HYGIENE PRACTICES? by Jacqueline M. Smith, RN, BN, Dyan B. Lokhorst, RN, CHPCN (C), BN (November, 2009) University of Calgary, Faculty of Nursing June, 2009Dokumen6 halamanINFECTION CONTROL: CAN NURSES IMPROVE HAND HYGIENE PRACTICES? by Jacqueline M. Smith, RN, BN, Dyan B. Lokhorst, RN, CHPCN (C), BN (November, 2009) University of Calgary, Faculty of Nursing June, 2009Rusida LiyaniBelum ada peringkat
- Preparing The Sterile Field PPT June 2011Dokumen61 halamanPreparing The Sterile Field PPT June 2011gerard_xucnBelum ada peringkat
- Thyroid Emergencies: Abrar AlharbiDokumen35 halamanThyroid Emergencies: Abrar AlharbiabrarBelum ada peringkat
- Patient's Bill of Rights PDFDokumen3 halamanPatient's Bill of Rights PDFPamela DizonBelum ada peringkat
- High-Risk Pregnancy Pregnancy-Induced Hypertension (PIH) What IsDokumen6 halamanHigh-Risk Pregnancy Pregnancy-Induced Hypertension (PIH) What IsJoe Anne Maniulit, MSN, RNBelum ada peringkat
- Safemotherhood 130212085105 Phpapp01Dokumen32 halamanSafemotherhood 130212085105 Phpapp01daniel laoatenBelum ada peringkat
- Fluid and Electrolyte Therapy - NCM 106Dokumen8 halamanFluid and Electrolyte Therapy - NCM 106Hana CyrilBelum ada peringkat
- Pediatric Concept MapDokumen12 halamanPediatric Concept Mapapi-352157080Belum ada peringkat
- Nursing ShortageDokumen10 halamanNursing Shortageالأغا محمد زكارنةBelum ada peringkat
- Intravenous Therapy Notes OnlineDokumen5 halamanIntravenous Therapy Notes OnlineDexie James Ventenilla DizonBelum ada peringkat
- Form 176 MDB (Updated Feb 2011)Dokumen19 halamanForm 176 MDB (Updated Feb 2011)Swati TyagiBelum ada peringkat
- Dental Scope of Practice GuideDokumen20 halamanDental Scope of Practice Guidearpita7dr9693Belum ada peringkat
- Manual RSSGH - 3 LevelsDokumen129 halamanManual RSSGH - 3 LevelsRyan Michael Oducado100% (1)
- TIME 2020 - ConsensoDokumen28 halamanTIME 2020 - ConsensoJacinta MontesBelum ada peringkat
- GYNAC Contact Update and Qualification TrackerDokumen4 halamanGYNAC Contact Update and Qualification TrackerAvinash ShrivastavaBelum ada peringkat
- 70037Dokumen4 halaman70037Nabila SaribanunBelum ada peringkat
- Atoosa Benji Resume 2016Dokumen3 halamanAtoosa Benji Resume 2016api-354834345Belum ada peringkat
- St. Peter's Hearst PavilionDokumen16 halamanSt. Peter's Hearst PavilionjmargalusBelum ada peringkat
- Shoulder Impingement RehabilitationDokumen3 halamanShoulder Impingement RehabilitationHamzh Sallam100% (2)
- Estrella, Christian R.: Education: Far Eastern University, 2010Dokumen3 halamanEstrella, Christian R.: Education: Far Eastern University, 2010Christian EstrellaBelum ada peringkat
- Pathogenesis and Etiology of Nasopharyngeal Carcinoma: Mu-Sheng Zeng and Yi-Xin ZengDokumen18 halamanPathogenesis and Etiology of Nasopharyngeal Carcinoma: Mu-Sheng Zeng and Yi-Xin ZengbarbiemeBelum ada peringkat
- Transdisciplinary Clinical Practice Between Physiotherapists and Traumatologists in Orthopaedic MedicineDokumen9 halamanTransdisciplinary Clinical Practice Between Physiotherapists and Traumatologists in Orthopaedic MedicineEnrique LopezBelum ada peringkat
- Genetics 9 10Dokumen41 halamanGenetics 9 10Anelya TurgambayevaBelum ada peringkat
- Normal Lower Limb Variants in ChildrenDokumen11 halamanNormal Lower Limb Variants in ChildrenIulia MoldovanBelum ada peringkat
- A New Current Obstetrics & Gynaecology: I. R. JohnsonDokumen1 halamanA New Current Obstetrics & Gynaecology: I. R. Johnsontirusew beleBelum ada peringkat
- Strengths and weaknesses of midwifery care from women's perspectivesDokumen9 halamanStrengths and weaknesses of midwifery care from women's perspectivesDita Rahmaika ABelum ada peringkat
- Resume FinalDokumen3 halamanResume Finalapi-452960406Belum ada peringkat
- Gastric Tube IrrigationDokumen3 halamanGastric Tube IrrigationRitika TandonBelum ada peringkat
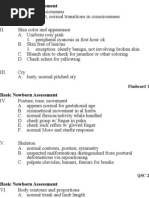
- Basic Newborn Assessment FlashcardsDokumen7 halamanBasic Newborn Assessment FlashcardsChristina Chaston MonteithBelum ada peringkat
- Rafa CVDokumen3 halamanRafa CVLou Dy SolisBelum ada peringkat
- Physiotherapy For ChildrenDokumen2 halamanPhysiotherapy For ChildrenCatalina LucaBelum ada peringkat
- Repertorium UniversaleDokumen13 halamanRepertorium Universaleatuguesp100% (1)
- HOGSI EU 2019 (Edited)Dokumen5 halamanHOGSI EU 2019 (Edited)Arie WidiyasaBelum ada peringkat
- Adventist StramaDokumen79 halamanAdventist Strama3132 ChicaBelum ada peringkat
- Awareness About Janani Shishu Suraksha Karyakram (JSSK) Among Pregnant Mothers - A Community Based Study in A Rural Area of West Bengal, India.Dokumen5 halamanAwareness About Janani Shishu Suraksha Karyakram (JSSK) Among Pregnant Mothers - A Community Based Study in A Rural Area of West Bengal, India.IOSRjournalBelum ada peringkat
- Color Atlas Minor SurgeryDokumen121 halamanColor Atlas Minor SurgeryRifQi KurniawanBelum ada peringkat
- What Is An Ibclc Flyer IlcaDokumen2 halamanWhat Is An Ibclc Flyer Ilcaapi-275110874Belum ada peringkat
- Breast Cancer Case Study: Answers For LifeDokumen4 halamanBreast Cancer Case Study: Answers For LifeFaye Mie VelascoBelum ada peringkat
- NMR Scan CentreDokumen4 halamanNMR Scan CentreDrNarayan KRBelum ada peringkat
- Course Aims: Nurses Nursing CareDokumen3 halamanCourse Aims: Nurses Nursing CareYen HuiBelum ada peringkat
- The Importance of Being Earnest: Classic Tales EditionDari EverandThe Importance of Being Earnest: Classic Tales EditionPenilaian: 4.5 dari 5 bintang4.5/5 (42)
- You Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherDari EverandYou Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherBelum ada peringkat
- Other People's Dirt: A Housecleaner's Curious AdventuresDari EverandOther People's Dirt: A Housecleaner's Curious AdventuresPenilaian: 3.5 dari 5 bintang3.5/5 (104)
- The Asshole Survival Guide: How to Deal with People Who Treat You Like DirtDari EverandThe Asshole Survival Guide: How to Deal with People Who Treat You Like DirtPenilaian: 4 dari 5 bintang4/5 (60)
- Welcome to the United States of Anxiety: Observations from a Reforming NeuroticDari EverandWelcome to the United States of Anxiety: Observations from a Reforming NeuroticPenilaian: 3.5 dari 5 bintang3.5/5 (10)
- Stephen Colbert's Midnight ConfessionsDari EverandStephen Colbert's Midnight ConfessionsPenilaian: 4 dari 5 bintang4/5 (125)
- The House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedDari EverandThe House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedPenilaian: 4.5 dari 5 bintang4.5/5 (5)
- Stiff: The Curious Lives of Human CadaversDari EverandStiff: The Curious Lives of Human CadaversPenilaian: 4 dari 5 bintang4/5 (3874)
- Sexual Bloopers: An Outrageous, Uncensored Collection of People's Most Embarrassing X-Rated FumblesDari EverandSexual Bloopers: An Outrageous, Uncensored Collection of People's Most Embarrassing X-Rated FumblesPenilaian: 3.5 dari 5 bintang3.5/5 (7)
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeDari EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifePenilaian: 4.5 dari 5 bintang4.5/5 (3)
- The Inimitable Jeeves [Classic Tales Edition]Dari EverandThe Inimitable Jeeves [Classic Tales Edition]Penilaian: 5 dari 5 bintang5/5 (3)
- Lessons from Tara: Life Advice from the World's Most Brilliant DogDari EverandLessons from Tara: Life Advice from the World's Most Brilliant DogPenilaian: 4.5 dari 5 bintang4.5/5 (42)
- The Smartest Book in the World: A Lexicon of Literacy, A Rancorous Reportage, A Concise Curriculum of CoolDari EverandThe Smartest Book in the World: A Lexicon of Literacy, A Rancorous Reportage, A Concise Curriculum of CoolPenilaian: 4 dari 5 bintang4/5 (14)
- Spoiler Alert: You're Gonna Die: Unveiling Death One Question at a TimeDari EverandSpoiler Alert: You're Gonna Die: Unveiling Death One Question at a TimePenilaian: 4 dari 5 bintang4/5 (56)
- Humorous American Short Stories: Selections from Mark Twain, O. Henry, James Thurber, Kurt Vonnegut, Jr. and moreDari EverandHumorous American Short Stories: Selections from Mark Twain, O. Henry, James Thurber, Kurt Vonnegut, Jr. and moreBelum ada peringkat
- The Comedians in Cars Getting Coffee BookDari EverandThe Comedians in Cars Getting Coffee BookPenilaian: 4.5 dari 5 bintang4.5/5 (8)
- The Hunger But Mainly Death Games: A ParodyDari EverandThe Hunger But Mainly Death Games: A ParodyPenilaian: 4 dari 5 bintang4/5 (9)