Anda mungkin juga menyukai
- About The NBCOT OTR and Cota Exams: Exam BasicsDokumen2 halamanAbout The NBCOT OTR and Cota Exams: Exam BasicsJennifer gomezBelum ada peringkat
- Pediatric Outcome MeasuresDokumen40 halamanPediatric Outcome MeasuresMaybelle Anne ZamoraBelum ada peringkat
- Jrooz Review Center: Tried and Tested Tips For The IELTS ExamDokumen12 halamanJrooz Review Center: Tried and Tested Tips For The IELTS ExamJameston BostreBelum ada peringkat
- The Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeDokumen55 halamanThe Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeAswathi100% (2)
- Assessing Functional AbilityDokumen15 halamanAssessing Functional AbilitySonali Soumyashree100% (2)
- 2012 Practice Analysis Executive Otr PDFDokumen32 halaman2012 Practice Analysis Executive Otr PDFRuxandra PredaBelum ada peringkat
- Battery TestsDokumen40 halamanBattery TestsStratiatella Faith Anthony100% (1)
- Assess Cognitive FunctioningDokumen9 halamanAssess Cognitive FunctioningIntan Indah Sari100% (2)
- Study ResourcesDokumen3 halamanStudy Resourcesapi-405162391Belum ada peringkat
- FIM ManualDokumen24 halamanFIM ManualAnshuman MihirBelum ada peringkat
- ABA Vs RDIDokumen6 halamanABA Vs RDIbugzibBelum ada peringkat
- Motor LearningDokumen3 halamanMotor LearningAndrea SantosBelum ada peringkat
- Home Environmental AssessmentDokumen2 halamanHome Environmental AssessmentSelvi Puspa SariBelum ada peringkat
- New Roods ApprochDokumen50 halamanNew Roods ApprochMonicca GV100% (1)
- Clients Goals To Address in SessionDokumen8 halamanClients Goals To Address in Sessionapi-436429414Belum ada peringkat
- Soap 11Dokumen4 halamanSoap 11api-436429414Belum ada peringkat
- OT Self Care Modified Barthel IndexDokumen4 halamanOT Self Care Modified Barthel Indexlolocy LBelum ada peringkat
- A Case Study On Task Oriented ApproachDokumen48 halamanA Case Study On Task Oriented ApproachTIMOTHY NYONGESA0% (1)
- Instrumental Activities Daily Living: Try ThisDokumen11 halamanInstrumental Activities Daily Living: Try ThisbalryoBelum ada peringkat
- Strategies Used by Occupational Therapy To Maximize ADL IndependenceDokumen53 halamanStrategies Used by Occupational Therapy To Maximize ADL IndependenceNizam lotfiBelum ada peringkat
- Pediatric Evaluation ReportDokumen3 halamanPediatric Evaluation Reportapi-469965619Belum ada peringkat
- Occupational Therapy in Pain ManagementDokumen26 halamanOccupational Therapy in Pain ManagementNoor Emellia JamaludinBelum ada peringkat
- Occupation Based InterventionsDokumen16 halamanOccupation Based Interventionsapi-293182319100% (1)
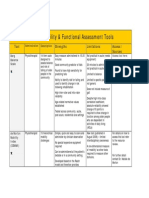
- Assessment Tools for Mobility & Functional IndependenceDokumen4 halamanAssessment Tools for Mobility & Functional Independencesonya63265Belum ada peringkat
- Chapter 16: Application of Motor Control and Motor LearningDokumen8 halamanChapter 16: Application of Motor Control and Motor LearningJireh Chambers100% (1)
- Aota PDFDokumen2 halamanAota PDFJuliana MassariolliBelum ada peringkat
- OT 101 NotesDokumen14 halamanOT 101 NotesAngeli Kyle Kaabay100% (1)
- Evaluation ReportDokumen3 halamanEvaluation Reportapi-547360536Belum ada peringkat
- Work and Occupational TherapyDokumen31 halamanWork and Occupational Therapysmith197077Belum ada peringkat
- Allen Cognitive Level Test Explained: History, Materials, AdministrationDokumen27 halamanAllen Cognitive Level Test Explained: History, Materials, AdministrationKimmy ChuBelum ada peringkat
- Math 7 Q4 Module 1Dokumen12 halamanMath 7 Q4 Module 1Joseph Agustin50% (4)
- Guidelines For Documentation of Occupational Therapy PDFDokumen7 halamanGuidelines For Documentation of Occupational Therapy PDFMaria AiramBelum ada peringkat
- Model of Human OccupationDokumen5 halamanModel of Human OccupationPatrick IlaoBelum ada peringkat
- Canadian Occupational Performance Measure (COPM) : 4 EditionDokumen3 halamanCanadian Occupational Performance Measure (COPM) : 4 EditionDulcea LoredanaBelum ada peringkat
- Occupational AdaptationDokumen5 halamanOccupational AdaptationVASH12345100% (1)
- LotcaDokumen165 halamanLotcaRica Salazar100% (5)
- Frame of ReferenceDokumen10 halamanFrame of ReferenceGustavo CabanasBelum ada peringkat
- Uniform Terminology AOTA PDFDokumen8 halamanUniform Terminology AOTA PDFLaura GuevaraBelum ada peringkat
- Occupational Therapy As A Major Activity of Human Being: by Rafia KhalidDokumen20 halamanOccupational Therapy As A Major Activity of Human Being: by Rafia Khalidnomi9818Belum ada peringkat
- TM Develop & Update Tour Ind Knowledge 310812Dokumen82 halamanTM Develop & Update Tour Ind Knowledge 310812Phttii phttii100% (1)
- Present Yourself SB L2-1Dokumen14 halamanPresent Yourself SB L2-1Hanan HabashiBelum ada peringkat
- OT Profile As A GuideDokumen8 halamanOT Profile As A GuideClara WangBelum ada peringkat
- Community Client Discharge SummaryDokumen3 halamanCommunity Client Discharge Summaryapi-271980676Belum ada peringkat
- Model of Human Occupation Parts 1-4Dokumen36 halamanModel of Human Occupation Parts 1-4Alice GiffordBelum ada peringkat
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionDari EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionBelum ada peringkat
- Motor Learning Theory: References: Cole & Tufano, Chapter 19 Reserve Article: Mathiowetz & Bass Haugen (1994) AJOTDokumen27 halamanMotor Learning Theory: References: Cole & Tufano, Chapter 19 Reserve Article: Mathiowetz & Bass Haugen (1994) AJOTSundar SweeBelum ada peringkat
- Occupational Therapy in Obsesive Compulsive DisorderDokumen3 halamanOccupational Therapy in Obsesive Compulsive DisorderManuela AlouBelum ada peringkat
- 2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)Dokumen54 halaman2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)engshi18Belum ada peringkat
- Occupational Therapy and Physical DysfunctionDokumen11 halamanOccupational Therapy and Physical DysfunctionM Burghal100% (2)
- The Learning Process: Definition and Perspective of LearningDokumen40 halamanThe Learning Process: Definition and Perspective of LearningMarjorie Ventuales Libo-onBelum ada peringkat
- LOTCA Assessment ReviewDokumen10 halamanLOTCA Assessment ReviewManik MishraBelum ada peringkat
- OTB 502 Syllabus 2019Dokumen22 halamanOTB 502 Syllabus 2019Gehan BotorsBelum ada peringkat
- GOALS Partnership-Occupational Therapist and Other Health ProfessionalsDokumen5 halamanGOALS Partnership-Occupational Therapist and Other Health ProfessionalsarvinBelum ada peringkat
- Eval Soap Note 2Dokumen9 halamanEval Soap Note 2api-435763096Belum ada peringkat
- Soap NoteDokumen2 halamanSoap Noteapi-285542134Belum ada peringkat
- Artifact 5 Soap NoteDokumen3 halamanArtifact 5 Soap Noteapi-517998988Belum ada peringkat
- Occupational Therapy ProcessDokumen3 halamanOccupational Therapy Processapi-339841373100% (1)
- Rabideau Kitchen Eval AjotDokumen8 halamanRabideau Kitchen Eval Ajotapi-291380671Belum ada peringkat
- OT and Eating DysfunctionDokumen1 halamanOT and Eating DysfunctionMCris EsSemBelum ada peringkat
- OT for LDs across Life CycleDokumen10 halamanOT for LDs across Life CycleLytiana WilliamsBelum ada peringkat
- Environmental Modifications: Nakul RangaDokumen42 halamanEnvironmental Modifications: Nakul Rangataniamahapatra1Belum ada peringkat
- Soap NoteDokumen1 halamanSoap Noteapi-519577267Belum ada peringkat
- Artifact 1 Case 3 UrsulaDokumen12 halamanArtifact 1 Case 3 Ursulaapi-517998988Belum ada peringkat
- Ota Group ProtocolDokumen26 halamanOta Group Protocolapi-318685839Belum ada peringkat
- 2 Introduction To TheoryDokumen14 halaman2 Introduction To TheoryNurul Izzah Wahidul AzamBelum ada peringkat
- Reflection of Good Governance in Sustainable Development: The Bangladesh ContextDokumen16 halamanReflection of Good Governance in Sustainable Development: The Bangladesh ContextSk ByBelum ada peringkat
- Guidelines For The USC Vol CorpsDokumen3 halamanGuidelines For The USC Vol CorpsAngeli GuadalupeBelum ada peringkat
- Marketing Graduate ProfileDokumen2 halamanMarketing Graduate Profilevkboss1301Belum ada peringkat
- Individual Student Profile-3Dokumen8 halamanIndividual Student Profile-3api-545465729Belum ada peringkat
- Math Operations Radicals-1 PDFDokumen2 halamanMath Operations Radicals-1 PDFTaj MartinBelum ada peringkat
- MGT-303 EntrepreneurshipDokumen10 halamanMGT-303 EntrepreneurshipAli Akbar MalikBelum ada peringkat
- Certificate in Advanced English: Alexandra-Elena GheorgheDokumen1 halamanCertificate in Advanced English: Alexandra-Elena GheorgheGheorghe AlexandraBelum ada peringkat
- NSEJS Exam DetailsDokumen3 halamanNSEJS Exam DetailsSaurabh JainBelum ada peringkat
- REVIEW OF RELATED LITERATURE - Docx JasminDokumen6 halamanREVIEW OF RELATED LITERATURE - Docx JasminRay Jefferson ValdonBelum ada peringkat
- Principles of Curriculum DevelopmentDokumen19 halamanPrinciples of Curriculum DevelopmentMichelleManguaMironBelum ada peringkat
- Brianna Nelson: Experience Aegis Coffee Roasters, 3630 Watson Hwy, Dubois - Barista Interests/HobbiesDokumen1 halamanBrianna Nelson: Experience Aegis Coffee Roasters, 3630 Watson Hwy, Dubois - Barista Interests/Hobbiesapi-459276311Belum ada peringkat
- Data Scientist-Novigo Solutions (5-7 Years' Experience) : Job DescriptionDokumen3 halamanData Scientist-Novigo Solutions (5-7 Years' Experience) : Job DescriptionKalyanKumarBelum ada peringkat
- Lesson-Plan-Voc Adjs Appearance Adjs PersonalityDokumen2 halamanLesson-Plan-Voc Adjs Appearance Adjs PersonalityHamza MolyBelum ada peringkat
- Newsletter 1982 460Dokumen12 halamanNewsletter 1982 460api-241041476Belum ada peringkat
- Session 1 Lesson 1: The Growing Up of Youth MinistryDokumen4 halamanSession 1 Lesson 1: The Growing Up of Youth MinistryMatheus Motta Dos SantosBelum ada peringkat
- Summer Class 2022 Grammar MaterialsDokumen12 halamanSummer Class 2022 Grammar MaterialsRuffa Coletoy AceroBelum ada peringkat
- Cover Letter: Subha Rajagopal 8248274315Dokumen7 halamanCover Letter: Subha Rajagopal 8248274315Yasi HanifBelum ada peringkat
- Micro TeachingDokumen14 halamanMicro TeachingChanlin ChackoBelum ada peringkat
- Ateneo Zamboanga Nursing FormsDokumen17 halamanAteneo Zamboanga Nursing FormsRyan MirandaBelum ada peringkat
- Assigment Strength of Material I Semester I Year IIIDokumen18 halamanAssigment Strength of Material I Semester I Year IIITeav PoliBelum ada peringkat
- MCQs On Amino Acids For NEET 2023 PDFDokumen1 halamanMCQs On Amino Acids For NEET 2023 PDFAli HassanBelum ada peringkat
- Study Guide: IGCSE and AS/A2 Level 2017 - 2018Dokumen45 halamanStudy Guide: IGCSE and AS/A2 Level 2017 - 2018Shakila ShakiBelum ada peringkat
- Edwards Groves 2014Dokumen12 halamanEdwards Groves 2014Camila LaraBelum ada peringkat
- AICB Compliance DPSDokumen7 halamanAICB Compliance DPSAravind Hades0% (1)
- EQ2410 (2E1436) Advanced Digital CommunicationsDokumen11 halamanEQ2410 (2E1436) Advanced Digital CommunicationsdwirelesBelum ada peringkat