Anda mungkin juga menyukai
- Pediatric Shock AWSDokumen77 halamanPediatric Shock AWSAsyiyatur RaudhahBelum ada peringkat
- Identifikasi RisikoDokumen0 halamanIdentifikasi RisikoShezye FaBelum ada peringkat
- Pancreatitis PD AnkDokumen13 halamanPancreatitis PD AnkAsyiyatur RaudhahBelum ada peringkat
- ProcitisDokumen7 halamanProcitisAsyiyatur RaudhahBelum ada peringkat
- ProcitisDokumen7 halamanProcitisAsyiyatur RaudhahBelum ada peringkat
- MDN Femoral Interlocking Recon Nail Intramedullary Fixation Metal Guide Surgical TechniqueDokumen28 halamanMDN Femoral Interlocking Recon Nail Intramedullary Fixation Metal Guide Surgical TechniqueAsyiyatur RaudhahBelum ada peringkat
- Osteomielitis PDFDokumen14 halamanOsteomielitis PDFAsyiyatur RaudhahBelum ada peringkat
- Human Body Muscles With Internal Organs Catalog Number: GD/A10001Dokumen3 halamanHuman Body Muscles With Internal Organs Catalog Number: GD/A10001Asyiyatur RaudhahBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- MCQsDokumen25 halamanMCQsdrstraoBelum ada peringkat
- Patellofemoral Pain After Total Knee Arthroplasty PDFDokumen8 halamanPatellofemoral Pain After Total Knee Arthroplasty PDFSergiu PlescaBelum ada peringkat
- Access Medicine - TableDokumen2 halamanAccess Medicine - Tablecode-24Belum ada peringkat
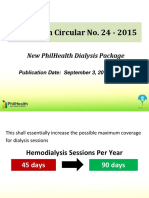
- 09 Dialysis DataDokumen11 halaman09 Dialysis DataThinkingPinoyBelum ada peringkat
- Colonic InertiaDokumen20 halamanColonic InertiaAndina Destiyani PutriBelum ada peringkat
- Resp TestDokumen7 halamanResp TestKong KongBelum ada peringkat
- Homeopathic Remedy Price List 2009-10Dokumen1 halamanHomeopathic Remedy Price List 2009-10yvranprasad100% (1)
- Constraints PDFDokumen4 halamanConstraints PDFArun Gopal100% (1)
- Management of Patients With Gastric and Duodenal DisordersDokumen47 halamanManagement of Patients With Gastric and Duodenal DisordersJor GarciaBelum ada peringkat
- Nursing Test Bank QuestionDokumen97 halamanNursing Test Bank QuestionADEDIRAN ABIONABelum ada peringkat
- Personal Trainer Magazine PDFDokumen54 halamanPersonal Trainer Magazine PDFdixieakerszBelum ada peringkat
- Upadacitinib Efficacy For The Treatment of Concomitant Psoriasis and Alopecia AreataDokumen4 halamanUpadacitinib Efficacy For The Treatment of Concomitant Psoriasis and Alopecia AreataAthenaeum Scientific PublishersBelum ada peringkat
- The Soulmate DietDokumen24 halamanThe Soulmate DietShana MarieBelum ada peringkat
- HAAD Exam For Nurses Questions 2018Dokumen46 halamanHAAD Exam For Nurses Questions 2018Asif Newaz100% (6)
- Body Condition Scoring As A Tool For Dairy Herd Management PDFDokumen5 halamanBody Condition Scoring As A Tool For Dairy Herd Management PDFfrankyBelum ada peringkat
- Pooja - 1Dokumen61 halamanPooja - 1Shobhit GoswamiBelum ada peringkat
- Psychometric Asssessment: A Psychometric Test Must BeDokumen8 halamanPsychometric Asssessment: A Psychometric Test Must BePoojaBelum ada peringkat
- Thyroglossal CystsDokumen4 halamanThyroglossal CystsCondurache Ilie-AndreiBelum ada peringkat
- ADHD in ChildrenDokumen16 halamanADHD in ChildrenCoco Hithere100% (1)
- Surgery MnemonicsDokumen6 halamanSurgery MnemonicsMarkoMilivojevic50% (2)
- Category-Wise Opening & Closing Rank-Ayur - BHU Int.Dokumen5 halamanCategory-Wise Opening & Closing Rank-Ayur - BHU Int.srikanth PosaBelum ada peringkat
- Yakima Co (WA) Protocols 2010Dokumen117 halamanYakima Co (WA) Protocols 2010Anthony James-Hartwell100% (1)
- Cervicogenic HeadacheDokumen32 halamanCervicogenic HeadacheasasakopBelum ada peringkat
- For Older People, Medications Are Common AGS Beers Criteria Aims To Make Them Appropriate, TooDokumen3 halamanFor Older People, Medications Are Common AGS Beers Criteria Aims To Make Them Appropriate, TooindriBelum ada peringkat
- Rehabilitation of Glossectomy Cases With Tongue Prosthesis: A Literature ReviewDokumen4 halamanRehabilitation of Glossectomy Cases With Tongue Prosthesis: A Literature ReviewmujtabaBelum ada peringkat
- Diarrhea CPDokumen8 halamanDiarrhea CPAsma SaleemBelum ada peringkat
- Case Group 1Dokumen10 halamanCase Group 1JASMEEN RAVALBelum ada peringkat
- Health Related Millennium Development Goals Part IDokumen24 halamanHealth Related Millennium Development Goals Part IGudegna GemechuBelum ada peringkat
- Temporomandibular Joint DisorderDokumen9 halamanTemporomandibular Joint DisorderTannels100% (1)
- Betamethasone (Drug Study)Dokumen4 halamanBetamethasone (Drug Study)Franz.thenurse6888100% (1)