Anda mungkin juga menyukai
- Current Recommendations For Diagnosis and Management of Polyoma BK Virus Nephropathy in Renal Transplant RecipientsDokumen4 halamanCurrent Recommendations For Diagnosis and Management of Polyoma BK Virus Nephropathy in Renal Transplant RecipientsAngelica GramaticuBelum ada peringkat
- Current Recommendations For Diagnosis and Management of Polyoma BK Virus Nephropathy in Renal Transplant RecipientsDokumen4 halamanCurrent Recommendations For Diagnosis and Management of Polyoma BK Virus Nephropathy in Renal Transplant RecipientsAngelica GramaticuBelum ada peringkat
- ACG Guideline Cdifficile April 2013Dokumen21 halamanACG Guideline Cdifficile April 2013Angelica GramaticuBelum ada peringkat
- NDT Ghid 2011Dokumen8 halamanNDT Ghid 2011Angelica GramaticuBelum ada peringkat
- Ecp2009 Precongress Transpl Path SvseshanDokumen40 halamanEcp2009 Precongress Transpl Path SvseshanAngelica GramaticuBelum ada peringkat
- 2400Dokumen7 halaman2400Angelica GramaticuBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Atlas of Procedure in Neonatology.2007.4th EdDokumen554 halamanAtlas of Procedure in Neonatology.2007.4th EdRamona Varzaru100% (4)
- KNUST EuniceDokumen8 halamanKNUST EuniceAngela Owusu SekyereBelum ada peringkat
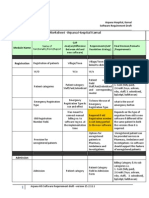
- Finalized Requirements-Worksheet - Arpana Hospital KarnalDokumen11 halamanFinalized Requirements-Worksheet - Arpana Hospital KarnalMahesh PatilBelum ada peringkat
- Orthodontic Products Online Magazine (Reliance Orthodontics L.E.D Pro Seal)Dokumen3 halamanOrthodontic Products Online Magazine (Reliance Orthodontics L.E.D Pro Seal)Reliance Orthodontic ProductsBelum ada peringkat
- ASPE Vol3 Chapter2 PDFDokumen56 halamanASPE Vol3 Chapter2 PDFAu C. GacotBelum ada peringkat
- OETDokumen16 halamanOETReina Anne JaymeBelum ada peringkat
- The GWAC Critical Care Chronicle 6-14Dokumen5 halamanThe GWAC Critical Care Chronicle 6-14gwacaacnBelum ada peringkat
- Benefits of The Costoclavicular Space For.15Dokumen2 halamanBenefits of The Costoclavicular Space For.15andrew herringBelum ada peringkat
- Using Routine Comparative Data To Assess The Quality of Health Care: Understanding and Avoiding Common PitfallsDokumen7 halamanUsing Routine Comparative Data To Assess The Quality of Health Care: Understanding and Avoiding Common Pitfallsujangketul62Belum ada peringkat
- Real Life, Real MiraclesDokumen27 halamanReal Life, Real MiraclesBethany House Publishers100% (1)
- Resume: Sub: Job For The Clnical Staff NurseDokumen6 halamanResume: Sub: Job For The Clnical Staff NurseJai SinghrandhawaBelum ada peringkat
- Palliative Care Practice and Associated Factors Among Nurses Working in Jimma University Medical Center South-West Ethiopia, 2017Dokumen8 halamanPalliative Care Practice and Associated Factors Among Nurses Working in Jimma University Medical Center South-West Ethiopia, 2017Diani Rista SariBelum ada peringkat
- St. Anthony'S College: Dr. Elisa B. Valdez, FPSPDokumen3 halamanSt. Anthony'S College: Dr. Elisa B. Valdez, FPSPEden Marie FranciscoBelum ada peringkat
- Ultrasound Room RdsDokumen2 halamanUltrasound Room RdsAhmed SherifBelum ada peringkat
- 3 RelationalmodelDokumen49 halaman3 RelationalmodelPengkuh Ardi NugrahaBelum ada peringkat
- General Scheme Rules For Jubilee Micro Cover 2023Dokumen1 halamanGeneral Scheme Rules For Jubilee Micro Cover 2023Africa Inuka Hospital UgunjaBelum ada peringkat
- Soobramoney v. Minister of HealthDokumen2 halamanSoobramoney v. Minister of HealthPfunzo Jeffrey MunyaiBelum ada peringkat
- Annexure A6-8 A4Dokumen15 halamanAnnexure A6-8 A4bathinsreenivasBelum ada peringkat
- Ballad Health Comment Submission 8-2-19Dokumen21 halamanBallad Health Comment Submission 8-2-19Anonymous COFJlahBelum ada peringkat
- ACS HMS User ManualDokumen19 halamanACS HMS User ManualEvans Corp100% (1)
- Prescribing Information For The Administration of AminophyllineDokumen2 halamanPrescribing Information For The Administration of AminophyllinekolperrBelum ada peringkat
- Delhi Govt Hospital List PDFDokumen3 halamanDelhi Govt Hospital List PDFLaura Brown100% (1)
- Foreign Body Airway ObstructionDokumen15 halamanForeign Body Airway ObstructionKristine Anne SorianoBelum ada peringkat
- Checklist Hip ExaminationDokumen7 halamanChecklist Hip ExaminationJavednBelum ada peringkat
- สอบเข้าม 1วิชาภาษาอังกฤษDokumen25 halamanสอบเข้าม 1วิชาภาษาอังกฤษLiwiny Siriporn90% (10)
- CC 14086Dokumen201 halamanCC 14086starykBelum ada peringkat
- Emergency Department: 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PMDokumen1 halamanEmergency Department: 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PM 7PMCyril Jane0% (1)
- For Your Tomorrow Anzacs Laid To Rest in India-Anzacs Laid To Rest in IndiaDokumen127 halamanFor Your Tomorrow Anzacs Laid To Rest in India-Anzacs Laid To Rest in IndiaIndpaediaBelum ada peringkat
- Gap Analysis in Internal Assessment Against National Accreditation Board For Hospitals Healthcare Providers NABH Standards in 200 Bedded Super Specialty Hospital Ijariie6515 PDFDokumen15 halamanGap Analysis in Internal Assessment Against National Accreditation Board For Hospitals Healthcare Providers NABH Standards in 200 Bedded Super Specialty Hospital Ijariie6515 PDFDeepali MeshramBelum ada peringkat
- ResumeDokumen3 halamanResumeMona Lydia DelinaBelum ada peringkat