Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Pernicious Oral Habits-1 PDFDokumen35 halamanPernicious Oral Habits-1 PDFWen Shu GohBelum ada peringkat
- Acute PancreatitisDokumen39 halamanAcute PancreatitisJm Bernardo100% (1)
- Final PPT Stomatognathic SysDokumen110 halamanFinal PPT Stomatognathic SysDevangana Das100% (2)
- Ebf 303 Environmental and Animal PhysiologyDokumen61 halamanEbf 303 Environmental and Animal PhysiologyAngela BrownBelum ada peringkat
- 5426 PDF PDFDokumen4 halaman5426 PDF PDFErsya MusLih AnshoriBelum ada peringkat
- Laryngo Broncho EsophagologyDokumen94 halamanLaryngo Broncho EsophagologyFrederick Mars UntalanBelum ada peringkat
- AllDokumen54 halamanAlladham bani younesBelum ada peringkat
- Handbook of Equine Respiratory EndosDokumen127 halamanHandbook of Equine Respiratory EndosIoana Corbu CostacheBelum ada peringkat
- Skill Training For Swallowing Rehabilitation inDokumen9 halamanSkill Training For Swallowing Rehabilitation invaleria posadaBelum ada peringkat
- Chewing Cycle and Neuromuscular MechanismDokumen13 halamanChewing Cycle and Neuromuscular Mechanismharshita parashar67% (3)
- 1 - Case Disfagia DisfoniaDokumen41 halaman1 - Case Disfagia DisfoniaMegan ShanzuBelum ada peringkat
- Evaluacion de La Deglucion en PCDokumen4 halamanEvaluacion de La Deglucion en PCRodrigo MoralesBelum ada peringkat
- Digestive System - STUDY GUIDEDokumen34 halamanDigestive System - STUDY GUIDEItsme ArrowBelum ada peringkat
- Quality of Life in Swallowing Disorders (SWAL-QOL)Dokumen11 halamanQuality of Life in Swallowing Disorders (SWAL-QOL)Paola Andrea Silva CastilloBelum ada peringkat
- Grand Rounds Index UTMB Otolaryngology Home PageDokumen12 halamanGrand Rounds Index UTMB Otolaryngology Home Pagegdudex118811Belum ada peringkat
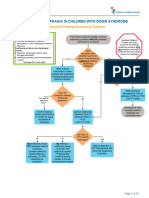
- Aspiration and Dysphagia in Children With Down SyndromeDokumen23 halamanAspiration and Dysphagia in Children With Down SyndromeJessa MaeBelum ada peringkat
- Maxillofacial Notes DR - Mahmoud RamadanDokumen83 halamanMaxillofacial Notes DR - Mahmoud Ramadanaziz200775% (4)
- Myology: The Buccinators Mechanism The TongueDokumen33 halamanMyology: The Buccinators Mechanism The TongueJee Arceo100% (1)
- Practice Standards AND Guidelines For Dysphagia Intervention by Speech-Language PathologistsDokumen38 halamanPractice Standards AND Guidelines For Dysphagia Intervention by Speech-Language PathologistsAlejandra Quezada GodoyBelum ada peringkat
- Digestion ResonanceDokumen52 halamanDigestion ResonanceEkta ManglaniBelum ada peringkat
- 1Dokumen8 halaman1EfanPutraBelum ada peringkat
- Wright 1966Dokumen17 halamanWright 1966Krupali Jain100% (1)
- DysphagiaDokumen4 halamanDysphagiaMicaBelum ada peringkat
- Gi PhysiologyDokumen21 halamanGi PhysiologyNoreen Orro BernalBelum ada peringkat
- 3 Digestive System RB CAGMAT REVIEW Anatomy and PhysiologyDokumen37 halaman3 Digestive System RB CAGMAT REVIEW Anatomy and PhysiologyFatima AbirinBelum ada peringkat
- Chapter-09 - Examination of Digestive SystemDokumen16 halamanChapter-09 - Examination of Digestive SystemAnnahi BcBelum ada peringkat
- Pemicu 1 DessyDokumen184 halamanPemicu 1 DessyDessy DsyBelum ada peringkat
- Nursing Care PlanDokumen8 halamanNursing Care PlanBiggs Juntilla100% (1)
- Dysphagia Evaluation Practices: Inconsistencies in Clinical Assessment and Instrumental Examination Decision-MakingDokumen12 halamanDysphagia Evaluation Practices: Inconsistencies in Clinical Assessment and Instrumental Examination Decision-MakingSamuel Morales NavarroBelum ada peringkat
- CH 26 Student DigestiveDokumen68 halamanCH 26 Student DigestiveMaski03Belum ada peringkat