Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Price List: Follow Us! @xdentallab @express Dental LaboratoryDokumen2 halamanPrice List: Follow Us! @xdentallab @express Dental LaboratoryHamidBelum ada peringkat
- Maxillofacial Injuries (3) / Orthodontic Courses by Indian Dental AcademyDokumen9 halamanMaxillofacial Injuries (3) / Orthodontic Courses by Indian Dental Academyindian dental academyBelum ada peringkat
- Lecture 17, Dental Implants (Script)Dokumen11 halamanLecture 17, Dental Implants (Script)JustDen09Belum ada peringkat
- PD Cen TR 12401-2009Dokumen14 halamanPD Cen TR 12401-2009gauravBelum ada peringkat
- 19 - 23 Gopu Chandran LPDokumen5 halaman19 - 23 Gopu Chandran LPBagis Emre GulBelum ada peringkat
- In Vitro Evaluation of Microleakage in Class LL Composite Restorations - High Viscosity Bulk-Fill Vs Conventional Composites 2019Dokumen7 halamanIn Vitro Evaluation of Microleakage in Class LL Composite Restorations - High Viscosity Bulk-Fill Vs Conventional Composites 2019Teo TeoBelum ada peringkat
- 2000 J. AqrabawiDokumen3 halaman2000 J. Aqrabawi謎超人Belum ada peringkat
- Unit 1.management of Flabby RidgeDokumen24 halamanUnit 1.management of Flabby RidgeLama NahedBelum ada peringkat
- Luting Cements and CementationDokumen59 halamanLuting Cements and CementationDRPRIYA007Belum ada peringkat
- American Dental Board of Prostodontics 2009Dokumen26 halamanAmerican Dental Board of Prostodontics 2009Roberto Puc100% (2)
- Transfer of Information For Esthetic and Functional Predictability in Severe Wear Cases.Dokumen11 halamanTransfer of Information For Esthetic and Functional Predictability in Severe Wear Cases.jorefe12Belum ada peringkat
- Prot OL: Sneak PeakDokumen32 halamanProt OL: Sneak PeakvictorBelum ada peringkat
- Complete DenturesDokumen44 halamanComplete DenturesChirag PatelBelum ada peringkat
- CHN - Oral - Health - Docx Filename - UTF-8''CHN Oral HealthDokumen7 halamanCHN - Oral - Health - Docx Filename - UTF-8''CHN Oral HealthYvonne Carmel Aguilar SunigaBelum ada peringkat
- HypercementosisDokumen4 halamanHypercementosisDian NoviaBelum ada peringkat
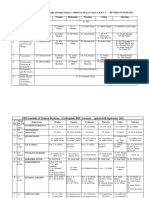
- Revised Schedule of BHU SSH OPD (Soft Copy) 2021Dokumen7 halamanRevised Schedule of BHU SSH OPD (Soft Copy) 2021rajubhagatssmBelum ada peringkat
- Landmark Studies in Periodontics - ISP WEBINARDokumen176 halamanLandmark Studies in Periodontics - ISP WEBINARvishrutha purushothamBelum ada peringkat
- OrthodonticsDokumen66 halamanOrthodonticsHady SpinBelum ada peringkat
- Mds Test 2 - RemovedDokumen92 halamanMds Test 2 - RemovedSubhashBelum ada peringkat
- Permanent CaninesDokumen4 halamanPermanent CaninesAmmar AwadBelum ada peringkat
- Dr. Razia Sultana: ContactDokumen5 halamanDr. Razia Sultana: ContactprasannaBelum ada peringkat
- Dental ImplantDokumen17 halamanDental ImplantGanesh GaneBelum ada peringkat
- OD Composite Class 3 Dan 4Dokumen2 halamanOD Composite Class 3 Dan 4Aniza Pratita SeptiadiniBelum ada peringkat
- Roth Polemica OrtodonciaDokumen6 halamanRoth Polemica OrtodonciaDavidBelum ada peringkat
- GC Tooth Mousse Effective Protection Against Caries and HypersensitivityDokumen7 halamanGC Tooth Mousse Effective Protection Against Caries and HypersensitivityNindya SulistyaniBelum ada peringkat
- 10 1016@j Bjoms 2020 04 011Dokumen5 halaman10 1016@j Bjoms 2020 04 011jamesBelum ada peringkat
- TFODokumen30 halamanTFOperiodontics07Belum ada peringkat
- Atraumatic Restorative Treatment (ART)Dokumen4 halamanAtraumatic Restorative Treatment (ART)solodont1Belum ada peringkat
- Bone Grafts and Substitutes in DentistryDokumen27 halamanBone Grafts and Substitutes in Dentistry林金鋒Belum ada peringkat
- Dawson 1Dokumen59 halamanDawson 1Hatem Ibrahim Ahmed AburiaBelum ada peringkat