Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Tenter 2000Dokumen42 halamanTenter 2000Mia BubankoBelum ada peringkat
- Cholesterol Blt00034 35 36 ADokumen2 halamanCholesterol Blt00034 35 36 AKERSYBelum ada peringkat
- Chloroquine Diphosphate Salt (C6628) - Product Information SheetDokumen1 halamanChloroquine Diphosphate Salt (C6628) - Product Information SheetSigma-Aldrich100% (2)
- Lymphocyte roles in immunologyDokumen13 halamanLymphocyte roles in immunologyDearma KhairunnisaBelum ada peringkat
- The Thalassemias and Hemolytic AnemiasDokumen43 halamanThe Thalassemias and Hemolytic AnemiasAnonymous elq7jZiSBelum ada peringkat
- Antibiotic Kill CurveDokumen2 halamanAntibiotic Kill CurveEdvinasStankūnasBelum ada peringkat
- Books To Follow For CSIR NET ExamDokumen3 halamanBooks To Follow For CSIR NET ExamAbhishek SinghBelum ada peringkat
- Proteomics: Technologies and Global MarketsDokumen5 halamanProteomics: Technologies and Global MarketsBCC ResearchBelum ada peringkat
- Dissertation Thomas Wieland - Next-Generation Sequencing Data AnalysisDokumen143 halamanDissertation Thomas Wieland - Next-Generation Sequencing Data AnalysisatpowrBelum ada peringkat
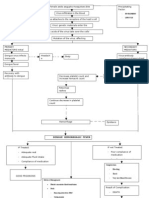
- Pathophysio DHF EDITEDDokumen3 halamanPathophysio DHF EDITEDricmichael100% (1)
- Vitamin K: Wallflower Sister of The FamousDokumen3 halamanVitamin K: Wallflower Sister of The FamousbisanpaBelum ada peringkat
- Syllabus-Neuroscience 10 Neuroscience in 21st Century-2012FallDokumen4 halamanSyllabus-Neuroscience 10 Neuroscience in 21st Century-2012FallJerikko Timm AgatepBelum ada peringkat
- Bioactive Natural Products Opportunities and Challenges in MedicinalDokumen695 halamanBioactive Natural Products Opportunities and Challenges in Medicinalney.barbosaBelum ada peringkat
- Biol 460 Case StudyDokumen11 halamanBiol 460 Case Studyapi-353888678Belum ada peringkat
- MRNA VaccineDokumen23 halamanMRNA VaccineIsworo RukmiBelum ada peringkat
- WJCC 8 1172Dokumen13 halamanWJCC 8 1172johoba5344Belum ada peringkat
- 11 - 12 1 Eiagen HTLV Ab Kit Rev131213Dokumen33 halaman11 - 12 1 Eiagen HTLV Ab Kit Rev131213Minesh VadsmiyaBelum ada peringkat
- Human CloningDokumen2 halamanHuman Cloningapi-318868666Belum ada peringkat
- Tips and Practical Plasma Applications.FDokumen45 halamanTips and Practical Plasma Applications.FSorin RotaruBelum ada peringkat
- Molecular Networking As A Drug Discovery, Drug Metabolism, and Precision Medicine StrategyDokumen12 halamanMolecular Networking As A Drug Discovery, Drug Metabolism, and Precision Medicine StrategySam SonBelum ada peringkat
- Superparamagnetism: Limits and ApplicationsDokumen7 halamanSuperparamagnetism: Limits and ApplicationsNguyen VuBelum ada peringkat
- Oncology Revision Environmental Factors ScreeningDokumen299 halamanOncology Revision Environmental Factors ScreeningMourian AmanBelum ada peringkat
- Hille B-Second Edition (For Printing)Dokumen617 halamanHille B-Second Edition (For Printing)matuskacarlosBelum ada peringkat
- Cells of The Immune SystemDokumen38 halamanCells of The Immune SystemprabuBelum ada peringkat
- Yoga Tips For HairLossDokumen10 halamanYoga Tips For HairLossimvavBelum ada peringkat
- Seizure Disorders: Musupila.M DCM, Adgm, BSC Cs (Unza) 6 November 2019Dokumen26 halamanSeizure Disorders: Musupila.M DCM, Adgm, BSC Cs (Unza) 6 November 2019Emmanuel MukukaBelum ada peringkat
- 3 - Internal Regulation Quiz Review Biopsychology 2Dokumen4 halaman3 - Internal Regulation Quiz Review Biopsychology 2Shelita NisyaBelum ada peringkat
- 3a ReproductionDokumen25 halaman3a ReproductionThaarvena Retina100% (1)
- MPL6Dokumen2 halamanMPL6Daniel AgustinBelum ada peringkat
- Annex 3 - MedcertDokumen3 halamanAnnex 3 - MedcertFCBelum ada peringkat