Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Mass of Christ The Savior by Dan Schutte LyricsDokumen1 halamanMass of Christ The Savior by Dan Schutte LyricsMark Greg FyeFye II33% (3)
- Penicillin Allergy: Penicillin Allergy:: Gbs Unknown or Negative and No Obstetric Risk FactorsDokumen1 halamanPenicillin Allergy: Penicillin Allergy:: Gbs Unknown or Negative and No Obstetric Risk FactorsPeter SongBelum ada peringkat
- Osce FlowchartDokumen1 halamanOsce FlowchartPeter SongBelum ada peringkat
- Ambient Particulate Air Pollution and Daily Mortality inDokumen13 halamanAmbient Particulate Air Pollution and Daily Mortality inPeter SongBelum ada peringkat
- Neighbourhood Support Centre PolicyiiDokumen3 halamanNeighbourhood Support Centre PolicyiiPeter SongBelum ada peringkat
- Values - The Attitudes That We Think of As Justified and Connected With Our Emotions and What Makes Actions orDokumen4 halamanValues - The Attitudes That We Think of As Justified and Connected With Our Emotions and What Makes Actions orPeter SongBelum ada peringkat
- Aug 16. Aug: ZagrebDokumen2 halamanAug 16. Aug: ZagrebNat BrazBelum ada peringkat
- Classification and Use of LandDokumen5 halamanClassification and Use of LandShereenBelum ada peringkat
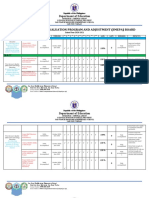
- SJDM Es Smepa Board 2020-2021Dokumen5 halamanSJDM Es Smepa Board 2020-2021Loreto Capitli MoralesBelum ada peringkat
- Chapter 18Dokumen24 halamanChapter 18Baby KhorBelum ada peringkat
- Configuring Srewquid Proxy ServerDokumen4 halamanConfiguring Srewquid Proxy ServerPendekar BlankBelum ada peringkat
- MC - Unit 2Dokumen3 halamanMC - Unit 2pnpt2801Belum ada peringkat
- Company Profile 2018: However, The Cover Is ExcludedDokumen16 halamanCompany Profile 2018: However, The Cover Is ExcludedJimmy R. Mendoza LeguaBelum ada peringkat
- 137684-1980-Serrano v. Central Bank of The PhilippinesDokumen5 halaman137684-1980-Serrano v. Central Bank of The Philippinespkdg1995Belum ada peringkat
- William SantiagoDokumen5 halamanWilliam SantiagoSubhadip Das SarmaBelum ada peringkat
- Traditions and Encounters 3Rd Edition Bentley Test Bank Full Chapter PDFDokumen49 halamanTraditions and Encounters 3Rd Edition Bentley Test Bank Full Chapter PDFsinhhanhi7rp100% (7)
- Washington D.C. Healthcare Systems, Inc. and Jeffrey Thompson v. District of ColumbiaDokumen94 halamanWashington D.C. Healthcare Systems, Inc. and Jeffrey Thompson v. District of ColumbiaDonnie KnappBelum ada peringkat
- How To Cite Legal Materials PDFDokumen2 halamanHow To Cite Legal Materials PDFNadine AbenojaBelum ada peringkat
- A Brief History & Development of Banking in India and Its FutureDokumen12 halamanA Brief History & Development of Banking in India and Its FutureMani KrishBelum ada peringkat
- FILL OUT THE Application Form: Device Operating System ApplicationDokumen14 halamanFILL OUT THE Application Form: Device Operating System ApplicationNix ArcegaBelum ada peringkat
- LWB Manual PDFDokumen1 halamanLWB Manual PDFKhalid ZgheirBelum ada peringkat
- Business Plan FinalDokumen28 halamanBusiness Plan FinalErica Millicent TenecioBelum ada peringkat
- Assignment 10Dokumen2 halamanAssignment 10Kristina KittyBelum ada peringkat
- Affidavit of ExplanationDokumen2 halamanAffidavit of ExplanationGerwinBelum ada peringkat
- Unit 14 Opinion Full EssayDokumen1 halamanUnit 14 Opinion Full EssayQuân Lê ĐàoBelum ada peringkat
- Local Labor Complaint FormDokumen1 halamanLocal Labor Complaint FormYVONNE PACETEBelum ada peringkat
- H8 Pro: Pan & Tilt Wi-Fi CameraDokumen12 halamanH8 Pro: Pan & Tilt Wi-Fi CameravalladaresoscarBelum ada peringkat
- Final PPT of FTPDokumen29 halamanFinal PPT of FTPamansrivastava007Belum ada peringkat
- Legal Acctng CasesDokumen108 halamanLegal Acctng CasesJerry Barad SarioBelum ada peringkat
- Bromelia in Bolivia Key Chiquitania PDFDokumen10 halamanBromelia in Bolivia Key Chiquitania PDFthrashingoBelum ada peringkat
- Environmental Change and ComplexityDokumen7 halamanEnvironmental Change and ComplexityIffah Nadzirah100% (2)
- Employee Self Service ESS User Manual: Enterprise Resource Planning (ERP) ProjectDokumen57 halamanEmployee Self Service ESS User Manual: Enterprise Resource Planning (ERP) ProjectJorge CadornaBelum ada peringkat
- Exam 6 PrimariaDokumen5 halamanExam 6 PrimariaEdurne De Vicente PereiraBelum ada peringkat
- Basic Tax EnvironmentDokumen8 halamanBasic Tax EnvironmentPeregrin TookBelum ada peringkat
- Case LawsDokumen4 halamanCase LawsLalgin KurianBelum ada peringkat