Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Marginal Turbid Band and Light Blue Crest, Signs Observed in Magnifying Narrow-Band Imaging Endoscopy, Are Indicative of Gastric Intestinal MetaplasiaDokumen17 halamanMarginal Turbid Band and Light Blue Crest, Signs Observed in Magnifying Narrow-Band Imaging Endoscopy, Are Indicative of Gastric Intestinal MetaplasiaEnrique Moreno GonzálezBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Prognostic Value of Alpha Fetoprotein and Des Gamma Carboxy Prothrombin Responses in Patients With Hepatocellular Carcinoma Treated With TransarterialDokumen22 halamanPrognostic Value of Alpha Fetoprotein and Des Gamma Carboxy Prothrombin Responses in Patients With Hepatocellular Carcinoma Treated With TransarterialBlake_jjBelum ada peringkat
- Allelotypes of Lung Adenocarcinomas Featuring ALK Fusion Demonstrate Fewer Onco - and Suppressor Gene ChangesDokumen22 halamanAllelotypes of Lung Adenocarcinomas Featuring ALK Fusion Demonstrate Fewer Onco - and Suppressor Gene ChangesEnrique Moreno GonzálezBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Screening of Finnish RAD51C Founder Mutations in Prostate and Colorectal Cancer PatientsDokumen17 halamanScreening of Finnish RAD51C Founder Mutations in Prostate and Colorectal Cancer PatientsEnrique Moreno GonzálezBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Integrative Oncology For Breast Cancer Patients: Introduction of An Expert-Based ModelDokumen18 halamanIntegrative Oncology For Breast Cancer Patients: Introduction of An Expert-Based ModelEnrique Moreno GonzálezBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Let-7 miRNA-binding site polymorphism in the KRAS 3`UTR; colorectal cancer screening population prevalence and influence on clinical outcome in patients with metastatic colorectal cancer treated with 5-fluorouracil and oxaliplatin +/- cetuximabDokumen17 halamanLet-7 miRNA-binding site polymorphism in the KRAS 3`UTR; colorectal cancer screening population prevalence and influence on clinical outcome in patients with metastatic colorectal cancer treated with 5-fluorouracil and oxaliplatin +/- cetuximabEnrique Moreno GonzálezBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Overexpression of Snail Is Associated With Lymph Node Metastasis and Poor Prognosis in Patients With Gastric CancerDokumen24 halamanOverexpression of Snail Is Associated With Lymph Node Metastasis and Poor Prognosis in Patients With Gastric CancerEnrique Moreno GonzálezBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Mmunohistochemical Analysis Based Ep-ICD Subcellular Localization Index (ESLI) Is A Novel Marker For Metastatic Papillary Thyroid MicrocarcinomaDokumen18 halamanMmunohistochemical Analysis Based Ep-ICD Subcellular Localization Index (ESLI) Is A Novel Marker For Metastatic Papillary Thyroid MicrocarcinomaEnrique Moreno GonzálezBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Green Tea Consumption and Risk of Esophageal Cancer: A Meta-Analysis of Epidemiologic StudiesDokumen20 halamanGreen Tea Consumption and Risk of Esophageal Cancer: A Meta-Analysis of Epidemiologic StudiesEnrique Moreno GonzálezBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Overexpression of Snail Is Associated With Lymph Node Metastasis and Poor Prognosis in Patients With Gastric CancerDokumen24 halamanOverexpression of Snail Is Associated With Lymph Node Metastasis and Poor Prognosis in Patients With Gastric CancerEnrique Moreno GonzálezBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Pancreatic Cancer Circulating Tumour Cells Express A Cell Motility Gene Signature That Predicts Survival After SurgeryDokumen21 halamanPancreatic Cancer Circulating Tumour Cells Express A Cell Motility Gene Signature That Predicts Survival After SurgeryEnrique Moreno GonzálezBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Obesity Is An Independent Risk Factor For Pre-Transplant Portal Vein Thrombosis in Liver Recipients.Dokumen12 halamanObesity Is An Independent Risk Factor For Pre-Transplant Portal Vein Thrombosis in Liver Recipients.Enrique Moreno GonzálezBelum ada peringkat
- Keratin 8 Variants Are Infrequent in Patients With Alcohol-Related Liver Cirrhosis and Do Not Associate With Development of Hepatocellular CarcinomaDokumen14 halamanKeratin 8 Variants Are Infrequent in Patients With Alcohol-Related Liver Cirrhosis and Do Not Associate With Development of Hepatocellular CarcinomaEnrique Moreno GonzálezBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- PDGFRalpha/beta and VEGFR2 Polymorphisms in Colorectal Cancer: Incidence and Implications in Clinical OutcomeDokumen21 halamanPDGFRalpha/beta and VEGFR2 Polymorphisms in Colorectal Cancer: Incidence and Implications in Clinical OutcomeEnrique Moreno GonzálezBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Recipient and Donor Thrombophilia and The Risk of Portal Venous Thrombosis and Hepatic Artery Thrombosis in Liver RecipientsDokumen9 halamanRecipient and Donor Thrombophilia and The Risk of Portal Venous Thrombosis and Hepatic Artery Thrombosis in Liver RecipientsEnrique Moreno GonzálezBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Transplant International Special Issue: Abstracts of The 14th Congress of The European Society For Organ Transplantation Volume 22, Issue Supplement s2, Pages 95-222, August 2009Dokumen128 halamanTransplant International Special Issue: Abstracts of The 14th Congress of The European Society For Organ Transplantation Volume 22, Issue Supplement s2, Pages 95-222, August 2009Enrique Moreno GonzálezBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Transplant International Special Issue: Abstracts of The 14th Congress of The European Society For Organ Transplantation Volume 22, Issue Supplement s2, Pages 95-222, August 2009Dokumen145 halamanTransplant International Special Issue: Abstracts of The 14th Congress of The European Society For Organ Transplantation Volume 22, Issue Supplement s2, Pages 95-222, August 2009Enrique Moreno GonzálezBelum ada peringkat
- Chab MTO 8e Mod 2 Final QuizDokumen24 halamanChab MTO 8e Mod 2 Final Quizshawnas09100% (1)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Ria ImmunoassayDokumen10 halamanRia ImmunoassayDinkey SharmaBelum ada peringkat
- KARYOTYPEDokumen23 halamanKARYOTYPELucia AndreeaBelum ada peringkat
- Antibodies To Watch in 2019: Hélène Kaplon & Janice M. ReichertDokumen46 halamanAntibodies To Watch in 2019: Hélène Kaplon & Janice M. ReichertAjay KumarBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Forensic CaseDokumen2 halamanForensic CaseGenina Joy Atienza FusiBelum ada peringkat
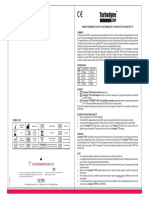
- Turbodyne: Tulip Diagnostics (P) LTDDokumen2 halamanTurbodyne: Tulip Diagnostics (P) LTDMatibar RahmanBelum ada peringkat
- Hyperparathyrodism Hypoparathyrodism: Dr. A. Wahyudi Pababbari, SPPD, FinasimDokumen48 halamanHyperparathyrodism Hypoparathyrodism: Dr. A. Wahyudi Pababbari, SPPD, FinasimKahfiyahBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- 269 - Embryology Physiology) Development of The Heart  - ÏDokumen11 halaman269 - Embryology Physiology) Development of The Heart  - ÏFood Safety CommunityBelum ada peringkat
- IgG Vs IgEDokumen2 halamanIgG Vs IgEvyasakandarpBelum ada peringkat
- Nurse Writing 003 OET Practice Letter by PASS OETDokumen26 halamanNurse Writing 003 OET Practice Letter by PASS OETNajad Salahudeen50% (2)
- Activity and ExerciseDokumen30 halamanActivity and ExerciseSIVA KRISHNA PRASAD ARJABelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Lab ReviewerDokumen3 halamanLab Reviewerryana cabreraBelum ada peringkat
- Chapter 43 - Thrombocytopenia and ThrombocytosisDokumen6 halamanChapter 43 - Thrombocytopenia and ThrombocytosisNathaniel SimBelum ada peringkat
- Brodsky 2004Dokumen14 halamanBrodsky 2004Ervan SuryaBelum ada peringkat
- IVMS Cell Biology and Pathology Flash Facts IDokumen4.999 halamanIVMS Cell Biology and Pathology Flash Facts IMarc Imhotep Cray, M.D.0% (2)
- Frog OrgansDokumen25 halamanFrog OrgansKen RubioBelum ada peringkat
- Private TutorialDokumen6 halamanPrivate TutorialHoàngQuýPhiBelum ada peringkat
- The Anatomy of Personality: The Lessons of Psychosurgery: - Prefrontal Leucotomy (By 1937)Dokumen14 halamanThe Anatomy of Personality: The Lessons of Psychosurgery: - Prefrontal Leucotomy (By 1937)LouBelum ada peringkat
- Electric Properties of Cardiac MusclesDokumen5 halamanElectric Properties of Cardiac Musclesragulkutty72Belum ada peringkat
- Tau-Targeting Antisense Oligonucleotide Mapt in Mild Alzheimer's Disease: A Phase 1b, Randomized, Placebo-Controlled TrialDokumen20 halamanTau-Targeting Antisense Oligonucleotide Mapt in Mild Alzheimer's Disease: A Phase 1b, Randomized, Placebo-Controlled TrialSiddharth NarsipurBelum ada peringkat
- INR Price List Sep22Dokumen60 halamanINR Price List Sep22YauBelum ada peringkat
- Lesson 4 Infancy by HurlockDokumen44 halamanLesson 4 Infancy by HurlockJessica Recaido100% (1)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Laughter Is Best Essay OtherDokumen2 halamanLaughter Is Best Essay OtherArchana SharmaBelum ada peringkat
- Genetic Influences in Human BehaviorDokumen24 halamanGenetic Influences in Human BehaviorGuillermo ArriagaBelum ada peringkat
- Eating Disorders: The Cause and Effect of MedicalizationDokumen6 halamanEating Disorders: The Cause and Effect of MedicalizationhaleeboppBelum ada peringkat
- ASNC AND EANM Amyloidosis Practice Points WEBDokumen12 halamanASNC AND EANM Amyloidosis Practice Points WEBElena FlorentinaBelum ada peringkat
- Exchange Blood Transfusion 2Dokumen15 halamanExchange Blood Transfusion 2Sarah100% (1)
- Fusidic AcidDokumen3 halamanFusidic AcidAusaf AhmadBelum ada peringkat
- Need To Know.: Self-Regulation: Science BackgrounderDokumen3 halamanNeed To Know.: Self-Regulation: Science BackgrounderRachelBelum ada peringkat
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (5)