Anda mungkin juga menyukai
- PT2 - Female MindDokumen70 halamanPT2 - Female MindAhmetBelum ada peringkat
- Sound, Frequency and Healing PresentationDokumen33 halamanSound, Frequency and Healing PresentationRalucaLaneve100% (4)
- METCON-5 Training ManualDokumen33 halamanMETCON-5 Training Manualbart140094% (16)
- Pamela J. Carter, Amy Stegen Lippincotts Advanced Skills For Nursing Assistants A Humanistic Approach To Caregiving PDFDokumen416 halamanPamela J. Carter, Amy Stegen Lippincotts Advanced Skills For Nursing Assistants A Humanistic Approach To Caregiving PDFMahmoud AbdallaBelum ada peringkat
- Chapter 27 GuytonDokumen6 halamanChapter 27 GuytonGabriella ChafrinaBelum ada peringkat
- M - 126 Structure of Nephron and Function of The Kidney PDFDokumen4 halamanM - 126 Structure of Nephron and Function of The Kidney PDFDr. Tapan Kr. Dutta100% (1)
- Pharmacology of Renal SystemDokumen125 halamanPharmacology of Renal SystemBirhanu GetaBelum ada peringkat
- Urinary Tract ReciewDokumen5 halamanUrinary Tract ReciewRobert LotzerBelum ada peringkat
- 6-Drugs Acting On The Renal System - 2Dokumen65 halaman6-Drugs Acting On The Renal System - 2Hamid Hussain HamidBelum ada peringkat
- 7,8-Handling of Na+ & Glucose by The Renal TubulesDokumen11 halaman7,8-Handling of Na+ & Glucose by The Renal TubulesOsama MohamedBelum ada peringkat
- Counter Current MechanismDokumen33 halamanCounter Current MechanismPhysiology by Dr Raghuveer67% (3)
- Reverse Osmosis Treatment of Drinking WaterDari EverandReverse Osmosis Treatment of Drinking WaterPenilaian: 3.5 dari 5 bintang3.5/5 (4)
- DP Biology - Speciation Lesson PlanDokumen2 halamanDP Biology - Speciation Lesson Planapi-257190713100% (1)
- Tubular ReabsorptionDokumen42 halamanTubular Reabsorptionmina mounirBelum ada peringkat
- Renal FunctionDokumen2 halamanRenal FunctionlenoBelum ada peringkat
- L4 Regional Transport 2023Dokumen4 halamanL4 Regional Transport 2023bgj9cddvxhBelum ada peringkat
- DCT and Collecting DuctDokumen29 halamanDCT and Collecting DuctayeshaBelum ada peringkat
- Handling of Certain Important Solutes by The Renal Tubules: Prof./ Ibrahim Mohamady IbrahimDokumen39 halamanHandling of Certain Important Solutes by The Renal Tubules: Prof./ Ibrahim Mohamady IbrahimOsama MohamedBelum ada peringkat
- Renal Physiology BY Dr. Olasupo. S. AdeniyiDokumen6 halamanRenal Physiology BY Dr. Olasupo. S. AdeniyiUloko ChristopherBelum ada peringkat
- Physio 2Dokumen6 halamanPhysio 2Mohammad AlomariBelum ada peringkat
- Distal Convoluted Tubules, Counter Current Mechanism, MicturitionDokumen94 halamanDistal Convoluted Tubules, Counter Current Mechanism, MicturitionSarah BirechBelum ada peringkat
- Tubular Reabsorption and Secretion: by Dr. Rukhsana AnwarDokumen49 halamanTubular Reabsorption and Secretion: by Dr. Rukhsana AnwarZia PhotostateBelum ada peringkat
- SHS.108.Lect-10 Tubular ReabsorptionDokumen61 halamanSHS.108.Lect-10 Tubular ReabsorptionAzlan YasirBelum ada peringkat
- Renal Tubular TransportDokumen38 halamanRenal Tubular TransportAhmad KhanBelum ada peringkat
- L5&6-Tubular Reabsorption& SecretionDokumen38 halamanL5&6-Tubular Reabsorption& SecretionsairahhannahBelum ada peringkat
- L8water Balance and Concentrating and Diluting MechanismDokumen15 halamanL8water Balance and Concentrating and Diluting MechanismOsama MohamedBelum ada peringkat
- Reabsorption (Excretion Physiology)Dokumen28 halamanReabsorption (Excretion Physiology)Ayesha IqbalBelum ada peringkat
- Kidney 2 AdelinaVladDokumen65 halamanKidney 2 AdelinaVladGiorgos Doukas KaranasiosBelum ada peringkat
- LOOP OF HENLE (Modified)Dokumen25 halamanLOOP OF HENLE (Modified)Chuleha SethBelum ada peringkat
- Physiology Kidney ReviewDokumen8 halamanPhysiology Kidney ReviewJulie TranBelum ada peringkat
- Part 1 - US-Grade 4-BiochemistryDokumen34 halamanPart 1 - US-Grade 4-BiochemistryFarah Bashar Al-RawachyBelum ada peringkat
- Chapter 18 DIURETICSDokumen14 halamanChapter 18 DIURETICSAlexandra AlexaBelum ada peringkat
- Handling of Certain Important Solutes by The Renal TubulesDokumen14 halamanHandling of Certain Important Solutes by The Renal TubulesOsama MohamedBelum ada peringkat
- Countercurrent MultiplicationDokumen4 halamanCountercurrent MultiplicationMichael Briscoe100% (1)
- Kidney NotesDokumen5 halamanKidney Notesnad2samBelum ada peringkat
- Filtration at Rest: Retention of WaterDokumen19 halamanFiltration at Rest: Retention of WaterkoushiksarkerBelum ada peringkat
- L3 +L4 Renal System 2023Dokumen31 halamanL3 +L4 Renal System 2023mizare29gBelum ada peringkat
- Renal PhysiologyDokumen56 halamanRenal PhysiologyfinazkyaloBelum ada peringkat
- Activity 36 - Urinary Tubular Reabsorption and SecretionDokumen6 halamanActivity 36 - Urinary Tubular Reabsorption and SecretionKaren Joy MagbanuaBelum ada peringkat
- Tubular Reabsorption and SecretionDokumen21 halamanTubular Reabsorption and SecretionAhmad KhanBelum ada peringkat
- PHS RenalDokumen44 halamanPHS Renaltewogbadeomobuwajo005Belum ada peringkat
- Excretion in MammalsDokumen17 halamanExcretion in MammalsKaynat JavedBelum ada peringkat
- Urinalysis and Body FluidsDokumen54 halamanUrinalysis and Body FluidsabdishakurBelum ada peringkat
- Urine Formation and Its CompositionDokumen22 halamanUrine Formation and Its CompositionZahidKhanBelum ada peringkat
- Drugs Affecting Renal FunctionDokumen52 halamanDrugs Affecting Renal Functionliakot prantoBelum ada peringkat
- Excretion IDokumen27 halamanExcretion Ierinjoy77Belum ada peringkat
- After Studying This Chapter, Students Should Be Able To - .Dokumen59 halamanAfter Studying This Chapter, Students Should Be Able To - .Deepika MahajanBelum ada peringkat
- Cicm Part 1 StudyDokumen6 halamanCicm Part 1 StudyReesha CornelioBelum ada peringkat
- REN Revision LectureDokumen43 halamanREN Revision Lecturegyamfi.rolandBelum ada peringkat
- What Are AntibioticsDokumen29 halamanWhat Are AntibioticsLouie BruanBelum ada peringkat
- Chapter 19 - The Urinary System: Fluid and Electrolyte BalanceDokumen28 halamanChapter 19 - The Urinary System: Fluid and Electrolyte BalanceSara SabraBelum ada peringkat
- DiureticsDokumen12 halamanDiureticslandita683Belum ada peringkat
- Blood Filtration and Nutrient and Water ReabsorptionDokumen2 halamanBlood Filtration and Nutrient and Water ReabsorptionNadia SalwaniBelum ada peringkat
- Diuretics: Pranjal Wagh Master of Pharmacy (2021-2023) Poona College of PharmacyDokumen39 halamanDiuretics: Pranjal Wagh Master of Pharmacy (2021-2023) Poona College of PharmacyPranjalBelum ada peringkat
- Distal Tubule Balance and Tubuloglomerular Feedback-Group 2Dokumen42 halamanDistal Tubule Balance and Tubuloglomerular Feedback-Group 2Chuleha SethBelum ada peringkat
- 1 DiurethicsDokumen8 halaman1 DiurethicsMoataz TrabehBelum ada peringkat
- THE URINARY SYSTEM Anatomy and PhysiologyDokumen29 halamanTHE URINARY SYSTEM Anatomy and PhysiologyYatuwa LydiaBelum ada peringkat
- Biokimia UrinDokumen2 halamanBiokimia UrinAswin AgusBelum ada peringkat
- Physio - Water BalanceDokumen8 halamanPhysio - Water Balanceavian_rose100% (2)
- NephronDokumen2 halamanNephronJohn SmithBelum ada peringkat
- Diuretics and Dialysis: DR Arpana HazarikaDokumen104 halamanDiuretics and Dialysis: DR Arpana HazarikaArpana HazarikaBelum ada peringkat
- APARATUL RenalDokumen38 halamanAPARATUL RenalElena SosuBelum ada peringkat
- GUS1-K6-Reabsorpsi & Sekresi TubulusDokumen33 halamanGUS1-K6-Reabsorpsi & Sekresi TubulusMarieta RitongaBelum ada peringkat
- Renal Physiology LatestDokumen63 halamanRenal Physiology LatestRaudzah RamliBelum ada peringkat
- The Urinary System 2013Dokumen52 halamanThe Urinary System 2013adystiBelum ada peringkat
- Robbins 14-18-19 NefrologieDokumen26 halamanRobbins 14-18-19 NefrologiejeskevandiemenBelum ada peringkat
- Ch. 18 Kidney and Urinary Tract Disorders.: ProteinuriaDokumen4 halamanCh. 18 Kidney and Urinary Tract Disorders.: ProteinuriajeskevandiemenBelum ada peringkat
- Rang Dale CirculatieDokumen19 halamanRang Dale CirculatiejeskevandiemenBelum ada peringkat
- Pathology CirculatieDokumen15 halamanPathology CirculatiejeskevandiemenBelum ada peringkat
- Rang and Dale's 14 - 22 - 25Dokumen7 halamanRang and Dale's 14 - 22 - 25jeskevandiemenBelum ada peringkat
- Robbins Ch15!16!17Dokumen26 halamanRobbins Ch15!16!17jeskevandiemenBelum ada peringkat
- Samenvatting Infectie en InflammatieDokumen169 halamanSamenvatting Infectie en InflammatiejeskevandiemenBelum ada peringkat
- Habitat and Adaptation - Grade 5Dokumen6 halamanHabitat and Adaptation - Grade 5Rasha GhabbounBelum ada peringkat
- Microfluidics: University of Ljubljana Faculty of Mathematics and Physics Department of PhysicsDokumen20 halamanMicrofluidics: University of Ljubljana Faculty of Mathematics and Physics Department of PhysicsMadhu MidhaBelum ada peringkat
- PH SalivaDokumen5 halamanPH SalivaBia KneippBelum ada peringkat
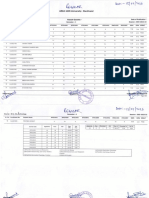
- Result Gazette Regular ODD 22 23 1st Semester B.SC Biotechnology. 1Dokumen2 halamanResult Gazette Regular ODD 22 23 1st Semester B.SC Biotechnology. 1Abhishek BhaduriBelum ada peringkat
- Lecture 3 Genetic CounselingDokumen23 halamanLecture 3 Genetic Counselingimorkzone100% (1)
- Infoprof Eng PDFDokumen158 halamanInfoprof Eng PDFacbgdvBelum ada peringkat
- Taurine 3 Cellular and Regulatory MechanismsDokumen510 halamanTaurine 3 Cellular and Regulatory MechanismsYoBjjBelum ada peringkat
- NPK Plant Basic DesignDokumen4 halamanNPK Plant Basic DesignDidier SanonBelum ada peringkat
- The Respiratory System: Lecture Presentation by Patty Bostwick-Taylor Florence-Darlington Technical CollegeDokumen30 halamanThe Respiratory System: Lecture Presentation by Patty Bostwick-Taylor Florence-Darlington Technical CollegeFakultas Kedokteran UnhanBelum ada peringkat
- Acute Pharyngitis in Children and Adolescents - Symptomatic Treatment UpToDateDokumen10 halamanAcute Pharyngitis in Children and Adolescents - Symptomatic Treatment UpToDateAaron VargasBelum ada peringkat
- S7 - Q2 - Summative Test 2Dokumen6 halamanS7 - Q2 - Summative Test 2Raniel LacuarinBelum ada peringkat
- Nursing Health History ReyDokumen10 halamanNursing Health History ReyNikki MarieBelum ada peringkat
- NutrigenomicsDokumen8 halamanNutrigenomicsGabriel MarcosBelum ada peringkat
- Dr. John's Mother Tinctures & Dilutions List Dr. John's Mother Tinctures & Dilutions ListDokumen6 halamanDr. John's Mother Tinctures & Dilutions List Dr. John's Mother Tinctures & Dilutions ListAnand KumarBelum ada peringkat
- Earl Eugene Castro - Bio 32 Learning Activity 1Dokumen2 halamanEarl Eugene Castro - Bio 32 Learning Activity 1EARL CASTROBelum ada peringkat
- Soma Devi InvoiceDokumen1 halamanSoma Devi InvoiceManeesh Verma100% (1)
- Biology Chapter 2 Sexual Reproduction in Flowering PlantsDokumen8 halamanBiology Chapter 2 Sexual Reproduction in Flowering PlantsYasir SalahBelum ada peringkat
- Bioinformatics PDFDokumen336 halamanBioinformatics PDFJoel CordeiroBelum ada peringkat
- Yield CalculationDokumen10 halamanYield CalculationrabinpadhanBelum ada peringkat
- Advanced Ecology Lab Final Exam by Roxanne UyDokumen9 halamanAdvanced Ecology Lab Final Exam by Roxanne Uyroxannediane@yahoo.com0% (1)
- Yoga Massage Therapy BookDokumen54 halamanYoga Massage Therapy BookKhadi MadamaBelum ada peringkat
- Stetson SpeechDokumen3 halamanStetson Speechjosiah9_5Belum ada peringkat
- Richard Ruvalcaba - The Successful Persons Guide To Time ManagementDokumen20 halamanRichard Ruvalcaba - The Successful Persons Guide To Time Managementapi-355177293Belum ada peringkat
- 11list2 23Dokumen1 halaman11list2 23yemocip111Belum ada peringkat
- North Rowan High School ProfileDokumen1 halamanNorth Rowan High School Profileapi-271352628Belum ada peringkat