Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Stress QuestionnaireDokumen2 halamanStress QuestionnaireCalin Popa100% (1)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- 3 2 1 Code It 5th Edition Green Test Bank 1Dokumen8 halaman3 2 1 Code It 5th Edition Green Test Bank 1elizabeth100% (32)
- 5 StsDokumen13 halaman5 StsPhooi Yee LauBelum ada peringkat
- Oconnelletal2017, Backpain GuildelineDokumen14 halamanOconnelletal2017, Backpain GuildelinePhooi Yee LauBelum ada peringkat
- Hu, ASLR Healthy PDFDokumen7 halamanHu, ASLR Healthy PDFPhooi Yee LauBelum ada peringkat
- Lumbar MultifidusDokumen6 halamanLumbar Multifidussridhar100% (1)
- Pre Operative Pelvis ExerciseDokumen1 halamanPre Operative Pelvis ExercisePhooi Yee LauBelum ada peringkat
- Colado, Athlete CoreDokumen9 halamanColado, Athlete CorePhooi Yee LauBelum ada peringkat
- Paillard PostureDokumen3 halamanPaillard PosturePhooi Yee LauBelum ada peringkat
- DiGiovanni 2003 PDFDokumen8 halamanDiGiovanni 2003 PDFPhooi Yee LauBelum ada peringkat
- RMQ English (Original)Dokumen2 halamanRMQ English (Original)Phooi Yee LauBelum ada peringkat
- Multom Rat Running PDFDokumen8 halamanMultom Rat Running PDFPhooi Yee LauBelum ada peringkat
- Neuro ExerciseDokumen7 halamanNeuro ExercisePhooi Yee LauBelum ada peringkat
- Humphreys, Cervicaloutcome For BalanceDokumen7 halamanHumphreys, Cervicaloutcome For BalancePhooi Yee LauBelum ada peringkat
- Plantartaping PDFDokumen2 halamanPlantartaping PDFPhooi Yee LauBelum ada peringkat
- Training To Optimize Performance Driving Reorganization?: Exercise and Functional in Stroke: NeuralDokumen10 halamanTraining To Optimize Performance Driving Reorganization?: Exercise and Functional in Stroke: NeuralPhooi Yee LauBelum ada peringkat
- Bourcher, NeckpainbalanceDokumen7 halamanBourcher, NeckpainbalancePhooi Yee LauBelum ada peringkat
- Urquhart, TR A PDFDokumen9 halamanUrquhart, TR A PDFPhooi Yee LauBelum ada peringkat
- DBE Movement PDFDokumen12 halamanDBE Movement PDFPhooi Yee LauBelum ada peringkat
- Dehner, NeckbalanceDokumen7 halamanDehner, NeckbalancePhooi Yee LauBelum ada peringkat
- Pinsault, Neck MuscleDokumen9 halamanPinsault, Neck MusclePhooi Yee LauBelum ada peringkat
- Frost, Low Back Pain BalanceDokumen7 halamanFrost, Low Back Pain BalancePhooi Yee LauBelum ada peringkat
- Merger, Eye MVTDokumen11 halamanMerger, Eye MVTPhooi Yee LauBelum ada peringkat
- Hellstrom, Neck SymphtaticDokumen15 halamanHellstrom, Neck SymphtaticPhooi Yee LauBelum ada peringkat
- Vuillerme, Cervical PostureDokumen5 halamanVuillerme, Cervical PosturePhooi Yee LauBelum ada peringkat
- Kogler, NeckbalanceDokumen6 halamanKogler, NeckbalancePhooi Yee LauBelum ada peringkat
- Kristenen, NeckmusclebalanceDokumen9 halamanKristenen, NeckmusclebalancePhooi Yee LauBelum ada peringkat
- Schimid - Neck Muscle PostureDokumen13 halamanSchimid - Neck Muscle PosturePhooi Yee LauBelum ada peringkat
- Yamagata, Neck ReflexDokumen4 halamanYamagata, Neck ReflexPhooi Yee LauBelum ada peringkat
- Kogler, NeckbalanceDokumen6 halamanKogler, NeckbalancePhooi Yee LauBelum ada peringkat
- Hellstrom, Neck SymphtaticDokumen15 halamanHellstrom, Neck SymphtaticPhooi Yee LauBelum ada peringkat
- Neuro Assessment ReportDokumen9 halamanNeuro Assessment Reportcosmic latte pulpsBelum ada peringkat
- Disabilties and Deformities in Leprosy Seminar14!4!2017Dokumen21 halamanDisabilties and Deformities in Leprosy Seminar14!4!2017Rohit GuptaBelum ada peringkat
- MRI Lumbar Spine Without ContrastDokumen2 halamanMRI Lumbar Spine Without ContrastMarco VincentiBelum ada peringkat
- Supercapsular Percutaneously Assisted Total Hip Arthroplasty For Osteoarthritis PDF 1899876162784453Dokumen6 halamanSupercapsular Percutaneously Assisted Total Hip Arthroplasty For Osteoarthritis PDF 1899876162784453JanetBelum ada peringkat
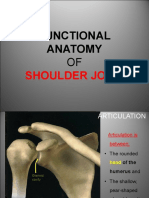
- Shoulder JointDokumen37 halamanShoulder JointsandeepBelum ada peringkat
- Gross B 2.20. Superficial Structures and Posterior Triangle of The NeckDokumen6 halamanGross B 2.20. Superficial Structures and Posterior Triangle of The NeckShaira Aquino VerzosaBelum ada peringkat
- Os Coxae: Pelvic Limb A. Os Coxae B. Femur C. D. Tarsals E. FDokumen4 halamanOs Coxae: Pelvic Limb A. Os Coxae B. Femur C. D. Tarsals E. FFor AstroBelum ada peringkat
- Knee Ligament InjuriesDokumen5 halamanKnee Ligament InjuriesNijin XmxBelum ada peringkat
- Pectoral Girdle Mcqs ExplainedDokumen12 halamanPectoral Girdle Mcqs ExplainedRobert Edwards100% (1)
- Clavicle FractureDokumen5 halamanClavicle FractureHasrul MuslihBelum ada peringkat
- Fetal PositionDokumen44 halamanFetal Positionjean therese100% (1)
- Ankle FracturesDokumen9 halamanAnkle FracturesUmar Dion SiraidBelum ada peringkat
- Mens.Health 男士完全健身手册 PDFDokumen25 halamanMens.Health 男士完全健身手册 PDFkcyapBelum ada peringkat
- Orthopedic Study Guide 2018Dokumen9 halamanOrthopedic Study Guide 2018Alif AllahBelum ada peringkat
- Acl InjuriesDokumen2 halamanAcl InjuriesFrnz RiveraBelum ada peringkat
- Anatomy of Stretching: Structural LimitationsDokumen5 halamanAnatomy of Stretching: Structural LimitationssdjuknicBelum ada peringkat
- Kyphosis Physiotherapy From Childhood To Old Age: Jean Claude de MauroyDokumen26 halamanKyphosis Physiotherapy From Childhood To Old Age: Jean Claude de MauroyromanciviBelum ada peringkat
- True NorthDokumen2 halamanTrue NorthtpBelum ada peringkat
- Subclavian ArteryDokumen8 halamanSubclavian ArteryPatalie HettihewaBelum ada peringkat
- Manual Muscle Test Handout by DR Chaman LalDokumen6 halamanManual Muscle Test Handout by DR Chaman LalChaman Lal KarotiaBelum ada peringkat
- Name: Rikki Mae P. Bueno Section: BSN-1105Dokumen1 halamanName: Rikki Mae P. Bueno Section: BSN-1105Rikki Mae BuenoBelum ada peringkat
- Case Study TKRDokumen22 halamanCase Study TKRInspirasi KhadijahBelum ada peringkat
- m2 What Is Sport AnalysisDokumen39 halamanm2 What Is Sport Analysisシファ ムスタファBelum ada peringkat
- Siemens MSK Ultrasound ImagingDokumen9 halamanSiemens MSK Ultrasound ImagingDehanBelum ada peringkat
- SpondyloarthritisDokumen77 halamanSpondyloarthritisRapid MedicineBelum ada peringkat
- Ballard - Written ExerciseDokumen2 halamanBallard - Written ExerciseJerald FernandezBelum ada peringkat
- McDillon, John - Weight Training for Beginners_ A Complete Illustrated Guide to Strenght Training at Home for Men and Women. Easy and Effective Exercises and Workouts with dumbbells to Burn Fat and Build MuscleDokumen74 halamanMcDillon, John - Weight Training for Beginners_ A Complete Illustrated Guide to Strenght Training at Home for Men and Women. Easy and Effective Exercises and Workouts with dumbbells to Burn Fat and Build MuscleabcdBelum ada peringkat
- Crisny Novika Yely Br. HutagaolDokumen3 halamanCrisny Novika Yely Br. Hutagaol20-221 Crisny Novika Yely Br. HutagaolBelum ada peringkat
- Knee MCL and LCL InjuriesDokumen90 halamanKnee MCL and LCL InjuriesImam SurkaniBelum ada peringkat