Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Deadly Deception - Robert WillnerDokumen303 halamanDeadly Deception - Robert Willnerleocarvalho001_60197100% (5)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Cast and SplintsDokumen58 halamanCast and SplintsSulabh Shrestha100% (2)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- What Is Malnutrition?: WastingDokumen6 halamanWhat Is Malnutrition?: WastingĐoan VõBelum ada peringkat
- Apraxia TreatmentDokumen80 halamanApraxia Treatmentaalocha_25100% (1)
- Sample Chapter of Assessment Made Incredibly Easy! 1st UK EditionDokumen28 halamanSample Chapter of Assessment Made Incredibly Easy! 1st UK EditionLippincott Williams and Wilkins- Europe100% (1)
- Bush y FrancisDokumen2 halamanBush y FrancisCarol Artigas100% (1)
- Páginas de Rockwood Fraturas em Adultos, 8ed3Dokumen51 halamanPáginas de Rockwood Fraturas em Adultos, 8ed3Estevão CananBelum ada peringkat
- Breast Imaging Review - A Quick Guide To Essential Diagnoses (2nd Edition) PDFDokumen264 halamanBreast Imaging Review - A Quick Guide To Essential Diagnoses (2nd Edition) PDFGregorio Parra100% (2)
- Oet Test Material: Occupational English Test Reading Sub-Test NursingDokumen13 halamanOet Test Material: Occupational English Test Reading Sub-Test NursingRyu Tse33% (3)
- Agarwal - Manual of Neuro OphthalmogyDokumen272 halamanAgarwal - Manual of Neuro Ophthalmogythycoon100% (4)
- CytokineDokumen26 halamanCytokinePro KartuBelum ada peringkat
- ACR-Global Hand Washing Day 2021Dokumen2 halamanACR-Global Hand Washing Day 2021Katy Chenee Napao Perez100% (1)
- Farming Hirudo LeechesDokumen46 halamanFarming Hirudo LeechesCatalin Cornel100% (1)
- Cytokeratin 7Dokumen12 halamanCytokeratin 7constantinilieBelum ada peringkat
- In Vitro Spheroid Model of Placental Vasculogenesis: Does It Work?Dokumen12 halamanIn Vitro Spheroid Model of Placental Vasculogenesis: Does It Work?constantinilieBelum ada peringkat
- Imunohisto PlacDokumen14 halamanImunohisto PlacconstantinilieBelum ada peringkat
- Plac Pathology - Drucilla RobertsDokumen11 halamanPlac Pathology - Drucilla RobertsconstantinilieBelum ada peringkat
- Ex - of - The - Hu - Plac 2003Dokumen8 halamanEx - of - The - Hu - Plac 2003constantinilieBelum ada peringkat
- Neuronal Survival in VitroDokumen29 halamanNeuronal Survival in VitroconstantinilieBelum ada peringkat
- Writing A Medical Paper PDFDokumen46 halamanWriting A Medical Paper PDFOctavian IancuBelum ada peringkat
- Pharyngeal ArchesDokumen35 halamanPharyngeal ArchesconstantinilieBelum ada peringkat
- Chapter 7 - Fractal GeometryDokumen15 halamanChapter 7 - Fractal GeometryzsuzannaBelum ada peringkat
- Newborn PaDokumen34 halamanNewborn PamarieBelum ada peringkat
- Plac Pathology - Drucilla RobertsDokumen11 halamanPlac Pathology - Drucilla RobertsconstantinilieBelum ada peringkat
- Placental PathologyDokumen39 halamanPlacental PathologyconstantinilieBelum ada peringkat
- EspidDokumen1 halamanEspidconstantinilieBelum ada peringkat
- GIT3 - Small, Large Surgical PathologyDokumen165 halamanGIT3 - Small, Large Surgical PathologyconstantinilieBelum ada peringkat
- Piscina in BerlinDokumen31 halamanPiscina in BerlinconstantinilieBelum ada peringkat
- GIT1 Surgical Pathology & X-RaysDokumen160 halamanGIT1 Surgical Pathology & X-Raysa4434431Belum ada peringkat
- Cardiovascular PathologyDokumen20 halamanCardiovascular PathologyconstantinilieBelum ada peringkat
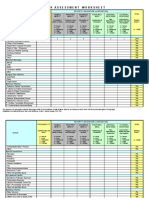
- IC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Dokumen4 halamanIC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Juon Vairzya AnggraeniBelum ada peringkat
- Formulation and Evaluation of Herbal Lip Rouge.: Research ArticleDokumen5 halamanFormulation and Evaluation of Herbal Lip Rouge.: Research ArticleTynBelum ada peringkat
- USA V Ronald Phillip Wallace Case 1:08-cr-00409-CMA Document 85 Filed 05/14/12 USDC ColoradoDokumen71 halamanUSA V Ronald Phillip Wallace Case 1:08-cr-00409-CMA Document 85 Filed 05/14/12 USDC ColoradoRob SBelum ada peringkat
- Hempseed As A Nutritional Resource: An Overview: J.C. CallawayDokumen8 halamanHempseed As A Nutritional Resource: An Overview: J.C. CallawayCarmen Yuliana GutierrezBelum ada peringkat
- UC San Diego: Independent Study ProjectsDokumen21 halamanUC San Diego: Independent Study ProjectsSoha ShahidBelum ada peringkat
- Drug StudyDokumen11 halamanDrug StudyKimberly Subade MandilagBelum ada peringkat
- Clinchers: RheumatologyDokumen22 halamanClinchers: RheumatologyvarrakeshBelum ada peringkat
- Tobacco Cessation PlanDokumen11 halamanTobacco Cessation PlanEsteban García EcheverryBelum ada peringkat
- Bahasa InggrisDokumen6 halamanBahasa InggrisSofi SusantoBelum ada peringkat
- Carbon Monoxide PoisoningDokumen31 halamanCarbon Monoxide PoisoningDheerajBelum ada peringkat
- University of Johannesburg MPH Reasearch Questionnaire Final Version JMDokumen9 halamanUniversity of Johannesburg MPH Reasearch Questionnaire Final Version JMYvonne MankolaBelum ada peringkat
- Reviewer in MCNDokumen16 halamanReviewer in MCNChristian Clyde Noel JakosalemBelum ada peringkat
- NCRP 160 PDFDokumen81 halamanNCRP 160 PDFmarkBelum ada peringkat
- Full Text of RA 7719Dokumen4 halamanFull Text of RA 7719camz_hernandezBelum ada peringkat
- Complications of DiabetesDokumen3 halamanComplications of Diabetesa7wfBelum ada peringkat
- ENGLISH 6 - Q4 - Wk7 - USLeM RTPDokumen11 halamanENGLISH 6 - Q4 - Wk7 - USLeM RTPtrishajilliene nacisBelum ada peringkat
- Menstrual Blood Derived Stem Cells and Their Scope in Regenerative Medicine A Review ArticleDokumen6 halamanMenstrual Blood Derived Stem Cells and Their Scope in Regenerative Medicine A Review ArticleInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat