Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Disaster NursingDokumen76 halamanDisaster Nursinghiral mistry100% (2)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Disaster NursingDokumen14 halamanDisaster Nursingangelogrande67% (3)
- Royal Hobart Mental Health Triage ScaleDokumen10 halamanRoyal Hobart Mental Health Triage ScaleJay UnniBelum ada peringkat
- Evidence Combination in Medical Data MiningDokumen5 halamanEvidence Combination in Medical Data MiningSasa TrifkovicBelum ada peringkat
- 0 2 1 6 IvanovicS MikinacDokumen10 halaman0 2 1 6 IvanovicS MikinacSasa TrifkovicBelum ada peringkat
- Data Mining in Medical Records For The Enhancement of Strategic Decisions: A Case StudyDokumen10 halamanData Mining in Medical Records For The Enhancement of Strategic Decisions: A Case StudySasa TrifkovicBelum ada peringkat
- Ijcse11 02 02 53Dokumen8 halamanIjcse11 02 02 53Sasa TrifkovicBelum ada peringkat
- InTech-Data Mining in NeurologyDokumen16 halamanInTech-Data Mining in NeurologySasa TrifkovicBelum ada peringkat
- Guidelines For First Responders To A CBRN IncidentDokumen16 halamanGuidelines For First Responders To A CBRN IncidentVon DominicBelum ada peringkat
- TRIAGE Skills LabDokumen8 halamanTRIAGE Skills Labczeremar chanBelum ada peringkat
- Triage PPT DownloadDokumen15 halamanTriage PPT DownloadEmergency ABMCBelum ada peringkat
- Triage in Emergency DepartmentDokumen27 halamanTriage in Emergency Departmentnaqibsakila4286Belum ada peringkat
- NABH-100 - FAQs 2013Dokumen11 halamanNABH-100 - FAQs 2013Priyanka Tudu100% (5)
- Disaster in Nursing 2Dokumen70 halamanDisaster in Nursing 2wulanBelum ada peringkat
- Practice Teaching On "Disaster Nursing"Dokumen10 halamanPractice Teaching On "Disaster Nursing"Rumela Ganguly ChakrabortyBelum ada peringkat
- PciDokumen3 halamanPciElizabeth PalacatBelum ada peringkat
- Triage Case StudyDokumen26 halamanTriage Case Studynadriyaasiin f.gBelum ada peringkat
- TriageDokumen84 halamanTriageMark Cheney100% (1)
- Esi (1Dokumen114 halamanEsi (1Ferina Mega SilviaBelum ada peringkat
- Determinant of Nurses' Response Time in Emergency Department When Taking Care of A PatientDokumen9 halamanDeterminant of Nurses' Response Time in Emergency Department When Taking Care of A PatientRuly AryaBelum ada peringkat
- Methodist Dallas Medical Center ExpansionDokumen6 halamanMethodist Dallas Medical Center ExpansionrappletonBelum ada peringkat
- Hospital PlanningDokumen8 halamanHospital PlanningadithiBelum ada peringkat
- NABH FAQ'sDokumen16 halamanNABH FAQ'sarun8591100% (1)
- CDP Assignment and Log TemplateDokumen2 halamanCDP Assignment and Log TemplateMichelle MorrisonBelum ada peringkat
- Triage Lecture DR F Mesa GaerlanDokumen55 halamanTriage Lecture DR F Mesa Gaerlanapi-19431894100% (1)
- Eddc Data Dictionary For Cherel Website 20170710Dokumen20 halamanEddc Data Dictionary For Cherel Website 20170710Sandro SperandeiBelum ada peringkat
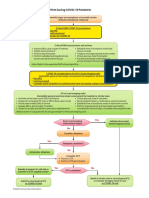
- Adult Suspected Stroke Algorithm During COVID-19 Pandemic: Yes NoDokumen1 halamanAdult Suspected Stroke Algorithm During COVID-19 Pandemic: Yes NoAnabel VinuezaBelum ada peringkat
- TriageDokumen20 halamanTriageIGDBelum ada peringkat
- Triage NurseDokumen1 halamanTriage NurseJeyser T. GamutiaBelum ada peringkat
- Edn Quiz 1 - A2: Questions 1 To 10Dokumen5 halamanEdn Quiz 1 - A2: Questions 1 To 10Je KirsteneBelum ada peringkat
- Disaster and Mass Casualty TriageDokumen3 halamanDisaster and Mass Casualty TriageNurul Fuady Fitryani AhmadBelum ada peringkat
- All One Hospital Command Center Employees/ StaffDokumen10 halamanAll One Hospital Command Center Employees/ StaffJudeLaxBelum ada peringkat
- ICN Disaster-Comp-Report WEB FinalDokumen16 halamanICN Disaster-Comp-Report WEB FinalSantoBelum ada peringkat
- Cristobal, Rocelyn P. MS Lec Post Task Triage FinalDokumen10 halamanCristobal, Rocelyn P. MS Lec Post Task Triage FinalRocelyn CristobalBelum ada peringkat
- 206.05 Aircraft Rescue Fire Fighting ResponsesDokumen12 halaman206.05 Aircraft Rescue Fire Fighting ResponsesijejwoirdwqowBelum ada peringkat