Anda mungkin juga menyukai
- Incident InvestDokumen16 halamanIncident InvestAndy DolmanBelum ada peringkat
- Incident InvestDokumen8 halamanIncident InvestAndy DolmanBelum ada peringkat
- Incident InvestDokumen16 halamanIncident InvestAndy DolmanBelum ada peringkat
- Quick checklist for incident investigatorsDokumen5 halamanQuick checklist for incident investigatorsAndy DolmanBelum ada peringkat
- Incident InvestDokumen15 halamanIncident InvestAndy DolmanBelum ada peringkat
- An Overview of Incident Causation TheoriesDokumen9 halamanAn Overview of Incident Causation TheoriesAndy DolmanBelum ada peringkat
- Continuous Improvement For The Incident Investigation SystemDokumen10 halamanContinuous Improvement For The Incident Investigation SystemAndy DolmanBelum ada peringkat
- Investigator Name: Event Assessed: Date of AssessmentDokumen1 halamanInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanBelum ada peringkat
- CCPS PS Beacon - Startup Hazards PDFDokumen1 halamanCCPS PS Beacon - Startup Hazards PDFDhanny MiharjaBelum ada peringkat
- Chemical Plant IncidentDokumen4 halamanChemical Plant Incidentsophiamaerelucio14Belum ada peringkat
- SPP101 Assignment 2: Environmental Management ApproachesDokumen6 halamanSPP101 Assignment 2: Environmental Management Approachesdarl1Belum ada peringkat
- IdipNEBOSH Unit A Past Exam QuestionsDokumen16 halamanIdipNEBOSH Unit A Past Exam Questionskrunalb@in89% (28)
- Root-Cause-Analysis (RCA) Best PracticeDokumen8 halamanRoot-Cause-Analysis (RCA) Best PracticeilbbeckBelum ada peringkat
- Lessons Learned 05 03Dokumen17 halamanLessons Learned 05 03NorthBelum ada peringkat
- Root Cause AnalysisDokumen19 halamanRoot Cause AnalysisMentari Putri PertiwiBelum ada peringkat
- IGC2 Examiner's ReportsDokumen18 halamanIGC2 Examiner's Reportssaqibsaeed18100% (6)
- Fertil Hazop StudyDokumen9 halamanFertil Hazop Studypkannan0% (1)
- Bab 13 Safety AuditDokumen51 halamanBab 13 Safety AuditR Muhammad FathiBelum ada peringkat
- Major Accident Investigation - How To Plan OneDokumen12 halamanMajor Accident Investigation - How To Plan Oneamineamine67Belum ada peringkat
- Managing A Condition Monitoring Program: Get The Monitoring Right!Dokumen9 halamanManaging A Condition Monitoring Program: Get The Monitoring Right!Michaelben Michaelben100% (1)
- UILS BBALLB Project Management CMT-311 FMEA Medical ExampleDokumen65 halamanUILS BBALLB Project Management CMT-311 FMEA Medical ExampleHarneet KaurBelum ada peringkat
- 6304 Journal U5Dokumen4 halaman6304 Journal U5sonndBelum ada peringkat
- 2008 Jan All - NoRestrictionDokumen24 halaman2008 Jan All - NoRestrictionRobertProsser19Belum ada peringkat
- Q A6 - Allocated Questions+AnsDokumen15 halamanQ A6 - Allocated Questions+Ansadishsewlall100% (1)
- Unit 4 PeeDokumen18 halamanUnit 4 PeePrabhamohanraj MohanrajBelum ada peringkat
- QMS 140 Root Cause Analysis Investigation Procedure SampleDokumen3 halamanQMS 140 Root Cause Analysis Investigation Procedure Samplex engineeringBelum ada peringkat
- Quality of Incident InvestigationsDokumen4 halamanQuality of Incident InvestigationsJose Martin ChaconBelum ada peringkat
- 2012 Tinga MBFA BookDokumen78 halaman2012 Tinga MBFA BookRushil RamroepBelum ada peringkat
- Process Safety in Chevron PDFDokumen40 halamanProcess Safety in Chevron PDFAndika Dimas Prinanda100% (1)
- Safety PDFDokumen25 halamanSafety PDFOkoli Chinedu ObioraBelum ada peringkat
- 3.2 HazopDokumen66 halaman3.2 Hazops sanjai100% (1)
- Shift Hand OverDokumen69 halamanShift Hand OverRestoration2010Belum ada peringkat
- FMEA Guide Failure ModesDokumen21 halamanFMEA Guide Failure ModesSusanoo12Belum ada peringkat
- Q-3 Define EIA. Elaborately Discuss Various Steps of EIA For The Successful Implementation of A Development ProjectDokumen3 halamanQ-3 Define EIA. Elaborately Discuss Various Steps of EIA For The Successful Implementation of A Development ProjectKeranigonj NewmarketBelum ada peringkat
- 2.20 PEIA_MEDIA0021Dokumen1 halaman2.20 PEIA_MEDIA0021Musaab MohamedBelum ada peringkat
- Safety Incidents in Ethylene PlantsDokumen21 halamanSafety Incidents in Ethylene PlantsDavid RodriguesBelum ada peringkat
- Process Safety Documentation OverviewDokumen5 halamanProcess Safety Documentation OverviewBadreddine BouzaraBelum ada peringkat
- TOR 2014 02202 Root Cause Investigation Best Practices GuideDokumen110 halamanTOR 2014 02202 Root Cause Investigation Best Practices GuideOCangaceiro100% (1)
- Maintain Safe Operations of Aging LNG FacilitiesDokumen40 halamanMaintain Safe Operations of Aging LNG FacilitiesAbu Faiz100% (1)
- Module3 Tkmit: Engineering As ExperimentationDokumen11 halamanModule3 Tkmit: Engineering As ExperimentationAnas A SBelum ada peringkat
- Continuous Improvement: A Corrective and Preventive Action (CAPA) PlanDokumen8 halamanContinuous Improvement: A Corrective and Preventive Action (CAPA) PlanEm NiaxBelum ada peringkat
- A Practical Approach To Managing Safety Critical Equipment and Systems in Process PlantsDokumen10 halamanA Practical Approach To Managing Safety Critical Equipment and Systems in Process Plantsfredo405Belum ada peringkat
- Osha 3895Dokumen3 halamanOsha 3895Kaycee Lyn Pablo BautistaBelum ada peringkat
- Chapter 3: Getting Started: Flow Chart - Implementation of Environmental Management of SystemDokumen9 halamanChapter 3: Getting Started: Flow Chart - Implementation of Environmental Management of Systemapi-3758747Belum ada peringkat
- Human Failure Capitulo 6Dokumen34 halamanHuman Failure Capitulo 6Fernando Alberto Sanguino ArellanoBelum ada peringkat
- 431 - 15 Exothermic ReactionsDokumen7 halaman431 - 15 Exothermic ReactionsAdriana Reyes Cordoba100% (1)
- Sw5a 059 TR 2 e e PDFDokumen44 halamanSw5a 059 TR 2 e e PDFAndrés MolinaBelum ada peringkat
- System Failure Analysis: Much Like The Work of A DetectiveDokumen8 halamanSystem Failure Analysis: Much Like The Work of A DetectiveKrishna BelelaBelum ada peringkat
- I. Terms: Property Damage or Is Worthy of RecordingDokumen4 halamanI. Terms: Property Damage or Is Worthy of RecordingKevin TabonaresBelum ada peringkat
- A Comparison of Three Types of Evacuation SystemDokumen20 halamanA Comparison of Three Types of Evacuation SystemKaimul BhuiyanBelum ada peringkat
- Risk Assessment FormDokumen2 halamanRisk Assessment FormYu JunanBelum ada peringkat
- Elements of PSM Terry Hardy.51145540Dokumen12 halamanElements of PSM Terry Hardy.51145540Syed Mujtaba Ali Bukhari100% (1)
- RefineriesDokumen273 halamanRefineriesLuis Santos100% (1)
- Weekend Shutdown of Validated AH SystemsDokumen4 halamanWeekend Shutdown of Validated AH SystemsPramoth NarashimmanBelum ada peringkat
- Flow Penanganan DeviasiDokumen4 halamanFlow Penanganan DeviasiGaluhBelum ada peringkat
- Dow Learnings and Actions From The Deepwater HorizonDokumen10 halamanDow Learnings and Actions From The Deepwater HorizonAbdul AwanBelum ada peringkat
- Alarms Management - Priority, Floods, Tears or Gain?: Introduction To The "Problem"Dokumen8 halamanAlarms Management - Priority, Floods, Tears or Gain?: Introduction To The "Problem"rbodewesBelum ada peringkat
- TPM Pillars & Improvement RoutesDokumen76 halamanTPM Pillars & Improvement RoutesYen NguyenBelum ada peringkat
- A Practical Guide For Behavioural Change in The Oil and Gas Industry.Dokumen65 halamanA Practical Guide For Behavioural Change in The Oil and Gas Industry.Cristina Rican100% (1)
- 2007 - An Overview of Trends in Aircraft Maintenance Program DevelopmentDokumen10 halaman2007 - An Overview of Trends in Aircraft Maintenance Program DevelopmentJorgeCanoRamirez100% (1)
- Incident InvestDokumen1 halamanIncident InvestAndy DolmanBelum ada peringkat
- Investigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Dokumen1 halamanInvestigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Andy DolmanBelum ada peringkat
- PSM Investigation Compliance ChecklistDokumen1 halamanPSM Investigation Compliance ChecklistAndy DolmanBelum ada peringkat
- Sample Formal Report Outline Incident Investigation GuidelineDokumen1 halamanSample Formal Report Outline Incident Investigation GuidelineAndy DolmanBelum ada peringkat
- Quick Checklist For Investigators: Physical ItemsDokumen4 halamanQuick Checklist For Investigators: Physical ItemsAndy DolmanBelum ada peringkat
- Investigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoDokumen1 halamanInvestigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoAndy DolmanBelum ada peringkat
- Investigator Name: Event Assessed: Date of AssessmentDokumen1 halamanInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanBelum ada peringkat
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDokumen1 halamanInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanBelum ada peringkat
- Checklist For Developing An Incident Investigation PlanDokumen1 halamanChecklist For Developing An Incident Investigation PlanAndy DolmanBelum ada peringkat
- Sample Investigation Improvement Checklist Incident Investigation GuidelineDokumen2 halamanSample Investigation Improvement Checklist Incident Investigation GuidelineAndy DolmanBelum ada peringkat
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDokumen1 halamanInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanBelum ada peringkat
- Flashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Dokumen8 halamanFlashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Andy DolmanBelum ada peringkat
- Investigator Name: Event Assessed: Date of AssessmentDokumen1 halamanInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanBelum ada peringkat
- Comprehensive List of CausesDokumen1 halamanComprehensive List of CausesAndy DolmanBelum ada peringkat
- Checklist To Prepare For An Inspection Incident Investigation GuidelineDokumen1 halamanChecklist To Prepare For An Inspection Incident Investigation GuidelineAndy DolmanBelum ada peringkat
- Customize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationDokumen4 halamanCustomize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationAndy DolmanBelum ada peringkat
- Propane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Dokumen2 halamanPropane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Andy DolmanBelum ada peringkat
- Relevant Organizations GuideDokumen3 halamanRelevant Organizations GuideAndy DolmanBelum ada peringkat
- Incident InvestDokumen5 halamanIncident InvestAndy DolmanBelum ada peringkat
- Appendix F: Selected OSHA and EPA Incident Investigation RegulationsDokumen3 halamanAppendix F: Selected OSHA and EPA Incident Investigation RegulationsAndy DolmanBelum ada peringkat
- Incident InvestDokumen1 halamanIncident InvestAndy DolmanBelum ada peringkat
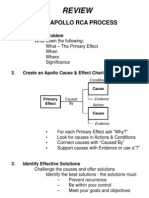
- Review: The Apollo Rca ProcessDokumen1 halamanReview: The Apollo Rca ProcessAndy DolmanBelum ada peringkat
- Appendix C: Photography Guidelines For Maximum ResultsDokumen3 halamanAppendix C: Photography Guidelines For Maximum ResultsAndy DolmanBelum ada peringkat
- Continuous Improvement For The Incident Investigation SystemDokumen10 halamanContinuous Improvement For The Incident Investigation SystemAndy DolmanBelum ada peringkat
- Appendix B: Professional Assistance DirectoryDokumen2 halamanAppendix B: Professional Assistance DirectoryAndy DolmanBelum ada peringkat
- Incident InvestDokumen17 halamanIncident InvestAndy DolmanBelum ada peringkat
- Incident InvestDokumen21 halamanIncident InvestAndy DolmanBelum ada peringkat
- Incident InvestDokumen17 halamanIncident InvestAndy DolmanBelum ada peringkat
- Feature: Writing Good Risk StatementsDokumen3 halamanFeature: Writing Good Risk StatementsenvisageBelum ada peringkat
- Application ControlDokumen16 halamanApplication ControlMeiliza Alayda UjmaBelum ada peringkat
- Develop Suppliers and Meet Quality StandardsDokumen41 halamanDevelop Suppliers and Meet Quality StandardsBalavignesh VenugopalBelum ada peringkat
- Branchless Banking in Pakistan: An Overview of Models and RegulationsDokumen11 halamanBranchless Banking in Pakistan: An Overview of Models and RegulationsSyed Ozair RizviBelum ada peringkat
- Cis ReviewerDokumen8 halamanCis ReviewerPhia TeoBelum ada peringkat
- House of Representatives Electoral TribunalDokumen21 halamanHouse of Representatives Electoral TribunalJunelBelum ada peringkat
- AtDokumen14 halamanAtInny AginBelum ada peringkat
- Iso 9001 Lead Auditorexam Preparation GuideDokumen15 halamanIso 9001 Lead Auditorexam Preparation Guidealoke gangulyBelum ada peringkat
- Fixed Asset Management Powerpoint PPT Template BundlesDokumen14 halamanFixed Asset Management Powerpoint PPT Template BundlesEuridídice ManuelBelum ada peringkat
- Audit Checklist in Production AreaDokumen5 halamanAudit Checklist in Production AreaPrince Moni100% (2)
- Guide On Cooperative Audit PDFDokumen25 halamanGuide On Cooperative Audit PDFNichole DouglasBelum ada peringkat
- Supplier Quality & Food Safety Audit: Your LogoDokumen6 halamanSupplier Quality & Food Safety Audit: Your LogokarupukamalBelum ada peringkat
- Tutorialanswer All QuestionsDokumen2.619 halamanTutorialanswer All QuestionsVolcanBlack100% (1)
- Coepd Exam 44 QuetionDokumen74 halamanCoepd Exam 44 Quetionphanindra pisipati100% (3)
- DefondDokumen17 halamanDefondLaksmi Mahendrati DwiharjaBelum ada peringkat
- IHCL SUBSIDIARY Annual Report 2009 10Dokumen348 halamanIHCL SUBSIDIARY Annual Report 2009 10raman86_netBelum ada peringkat
- Governance 29 May 06 PDFDokumen10 halamanGovernance 29 May 06 PDFrehanBelum ada peringkat
- Resume PKDokumen4 halamanResume PKBaljeetBelum ada peringkat
- Online ShoppingDokumen54 halamanOnline ShoppingVaryam Pandey50% (6)
- Audit Quality, Debt Financing, and Earnings Management - Evidence From JordanDokumen16 halamanAudit Quality, Debt Financing, and Earnings Management - Evidence From Jordantheresia dianBelum ada peringkat
- Female Directors May Reduce Earnings Management in Tech FirmsDokumen30 halamanFemale Directors May Reduce Earnings Management in Tech FirmsyockydockyBelum ada peringkat
- Arens Aud16 Inppt09Dokumen33 halamanArens Aud16 Inppt09euncieBelum ada peringkat
- CS-EnV-04 - Environmental Incident Management (01 16) - CS Energy RegisteredDokumen7 halamanCS-EnV-04 - Environmental Incident Management (01 16) - CS Energy RegisteredJohn EddyBelum ada peringkat
- Coursehero 12Dokumen2 halamanCoursehero 12nhbBelum ada peringkat
- CFASDokumen19 halamanCFASKuroko TetsuyaBelum ada peringkat
- 73 Curriculum Vitae FinanceDokumen1 halaman73 Curriculum Vitae FinanceExequiel AmbasingBelum ada peringkat
- Gaia Iar 2020Dokumen114 halamanGaia Iar 2020m_edas4262Belum ada peringkat
- Asset Integrity Intelligence: Mechanical Integrity Audit ChecklistDokumen14 halamanAsset Integrity Intelligence: Mechanical Integrity Audit ChecklistChris OpubaBelum ada peringkat
- Universal Standards On Social Performance ManagementDokumen21 halamanUniversal Standards On Social Performance ManagementTherese MarieBelum ada peringkat
- Auditing by BeasleyDokumen10 halamanAuditing by BeasleyElsa MendozaBelum ada peringkat