Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Critical Care NotesDokumen18 halamanCritical Care NotesjulieBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Preserving MeatDokumen16 halamanPreserving Meatfreemedic100% (2)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- CCRN-PCCN-CMC Review Cardiac Part 2Dokumen21 halamanCCRN-PCCN-CMC Review Cardiac Part 2Giovanni Mictil100% (1)
- Biochem I C System o 1894 CareDokumen458 halamanBiochem I C System o 1894 CareSteven Adams100% (4)
- Eating AcornsDokumen224 halamanEating Acornsapi-3707101100% (1)
- My Survival Gear by Tom Tindell: Flint KitDokumen3 halamanMy Survival Gear by Tom Tindell: Flint Kitfreemedic100% (1)
- Heart EditDokumen51 halamanHeart EditCoral Srinivasa Ramalu100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Size of Tackle: The First Thing To Know Is What: OR LeatherDokumen5 halamanSize of Tackle: The First Thing To Know Is What: OR Leatherelectricnusi100% (7)
- ACC Cardiovascular Board Review MCQ 2017Dokumen64 halamanACC Cardiovascular Board Review MCQ 2017Adeel Lakhiar100% (1)
- 6352 USN Phantoms in CombatDokumen66 halaman6352 USN Phantoms in Combatfreemedic100% (16)
- America S Greatest Special Ops Soldier Maj Dick MeadowsDokumen7 halamanAmerica S Greatest Special Ops Soldier Maj Dick MeadowsfreemedicBelum ada peringkat
- BOWIE KNIFE RevisitingBlackQuestionDokumen17 halamanBOWIE KNIFE RevisitingBlackQuestionfreemedicBelum ada peringkat
- Coarctation of Aorta (Paed)Dokumen18 halamanCoarctation of Aorta (Paed)NadiaMichu100% (1)
- Soldiers of The Napoleonic Wars #4 - Colours and Weapons - British Foot Guards at Waterloo, June 1815Dokumen26 halamanSoldiers of The Napoleonic Wars #4 - Colours and Weapons - British Foot Guards at Waterloo, June 1815J054663100% (7)
- Summative Test No. 2 Second Quarter Science 6Dokumen5 halamanSummative Test No. 2 Second Quarter Science 6BALETEBelum ada peringkat
- Past Years SNQ Answer by RCSIDokumen47 halamanPast Years SNQ Answer by RCSIhelamahjoubmounirdmo100% (1)
- Chinook Cargo SystemDokumen188 halamanChinook Cargo SystemfreemedicBelum ada peringkat
- Alss Aircrew Life SupportDokumen74 halamanAlss Aircrew Life SupportfreemedicBelum ada peringkat
- National Geographic Feb 2018Dokumen100 halamanNational Geographic Feb 2018Meor100% (2)
- Physiological Changes of Pregancy. NEW VERSION-For BSC Nursing StudentsDokumen107 halamanPhysiological Changes of Pregancy. NEW VERSION-For BSC Nursing StudentsKripa Susan100% (2)
- The Ukulele: A Magical History Tour: Bonus ChapterDokumen2 halamanThe Ukulele: A Magical History Tour: Bonus Chapterfreemedic0% (1)
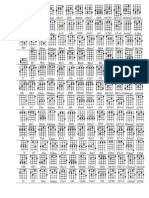
- C TuningDokumen1 halamanC TuningfreemedicBelum ada peringkat
- A Fieldbook of The StarsDokumen130 halamanA Fieldbook of The StarsLiam Glen MurdochBelum ada peringkat
- D TuningDokumen2 halamanD TuningfreemedicBelum ada peringkat
- C TuningDokumen1 halamanC TuningfreemedicBelum ada peringkat
- Fleabag SongbookDokumen14 halamanFleabag SongbookailopiBelum ada peringkat
- DtuningDokumen1 halamanDtuningtabayo_yatukishiBelum ada peringkat
- Blood TransfusionDokumen33 halamanBlood TransfusionfreemedicBelum ada peringkat
- World InstrumentsDokumen2 halamanWorld InstrumentsfreemedicBelum ada peringkat
- Chestsealinjury RevisedDokumen20 halamanChestsealinjury RevisedfreemedicBelum ada peringkat
- A Proposed Guideline For Tactical Medical Self-Care in The Civilian EnvironmentDokumen6 halamanA Proposed Guideline For Tactical Medical Self-Care in The Civilian EnvironmentfreemedicBelum ada peringkat
- Fleabag SongbookDokumen14 halamanFleabag SongbookailopiBelum ada peringkat
- Department of The Army Pyrotechnics Branch Aberdeen Proving Ground, Maryland 21020-5423Dokumen5 halamanDepartment of The Army Pyrotechnics Branch Aberdeen Proving Ground, Maryland 21020-5423freemedicBelum ada peringkat
- TC3 GuidelinesDokumen44 halamanTC3 Guidelinesfreemedic100% (1)
- TriageDokumen6 halamanTriagefreemedicBelum ada peringkat
- Point North CatalogDokumen84 halamanPoint North CatalogfreemedicBelum ada peringkat
- BeretsDokumen1 halamanBeretsfreemedic100% (1)
- Cold Water SurvivalDokumen2 halamanCold Water SurvivalfreemedicBelum ada peringkat
- Chapter 14Dokumen32 halamanChapter 14freemedicBelum ada peringkat
- WoodsmokeDokumen2 halamanWoodsmokefreemedicBelum ada peringkat
- Adobe Scan 13 May 2021Dokumen5 halamanAdobe Scan 13 May 2021Harisree SBelum ada peringkat
- Manual de Juguera de Acero Angel JuicerDokumen32 halamanManual de Juguera de Acero Angel JuicerFranco Benjamin Fernandez VasquezBelum ada peringkat
- What Is ECG?Dokumen2 halamanWhat Is ECG?Lê Thanh HàBelum ada peringkat
- Minoca AhjDokumen3 halamanMinoca AhjSundaresan SankarBelum ada peringkat
- Variability in The Hemodynamic Response To Fluid Bolus in Pediatric Septic Shock - 1Dokumen11 halamanVariability in The Hemodynamic Response To Fluid Bolus in Pediatric Septic Shock - 1diflopasBelum ada peringkat
- Pengaruh Terapi Rendam Kaki Dengan Air Hangat Terhadap Penurunan Tekanan Darah Pada Pasien Dengan Hipertensi Di Puskesmas Bahu ManadoDokumen8 halamanPengaruh Terapi Rendam Kaki Dengan Air Hangat Terhadap Penurunan Tekanan Darah Pada Pasien Dengan Hipertensi Di Puskesmas Bahu ManadoPutraBelum ada peringkat
- ECMO in Emergency SettingDokumen42 halamanECMO in Emergency Settingppds btkvBelum ada peringkat
- PhyseoDokumen7 halamanPhyseoRabiaNaseemBelum ada peringkat
- My CV in PDF File LDokumen115 halamanMy CV in PDF File LMohamed Omar ElfarokBelum ada peringkat
- HBP ReportDokumen2 halamanHBP ReportMindi May AguilarBelum ada peringkat
- Lifes Internal Secrets VDokumen23 halamanLifes Internal Secrets VYash PatelBelum ada peringkat
- 1 Cardiovascular SystemDokumen6 halaman1 Cardiovascular SystemWaltz PadlanBelum ada peringkat
- Heart and Breath SoundsDokumen9 halamanHeart and Breath Soundszeglam0% (1)
- Med 1 Block 2 - Wet Lab NotesDokumen36 halamanMed 1 Block 2 - Wet Lab NotesluckyBelum ada peringkat
- طب باطني نظري 5 مترجمةDokumen17 halamanطب باطني نظري 5 مترجمةali taroBelum ada peringkat
- Sub - Medical Surgical Nursing: Assignment On CVP MonitoringDokumen11 halamanSub - Medical Surgical Nursing: Assignment On CVP Monitoringkamini ChoudharyBelum ada peringkat
- ScenariosDokumen3 halamanScenarios3ternalBelum ada peringkat
- Circulatory System AssessmentDokumen4 halamanCirculatory System Assessmentapi-98991203Belum ada peringkat
- Abdominal Aortic AneurysmDokumen3 halamanAbdominal Aortic AneurysmRonald Cszar Fabian VillanoBelum ada peringkat
- HemodynamicsDokumen115 halamanHemodynamicsناصر دويكاتBelum ada peringkat