Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- DC Police Seek Persons of InterestDokumen140 halamanDC Police Seek Persons of InterestwtopwebBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Loudoun County Board of Supervisors Presentation - Early August 2020Dokumen21 halamanLoudoun County Board of Supervisors Presentation - Early August 2020wtopwebBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- 2020.06.09 Petition FinalsignedDokumen33 halaman2020.06.09 Petition FinalsignedwtopwebBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Bowser Letter To Operation Warp Speed 12-3-2020Dokumen2 halamanBowser Letter To Operation Warp Speed 12-3-2020wtopwebBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
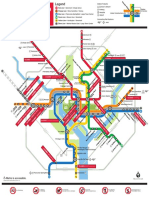
- 2019 System Map COVID-19 Stations FINALDokumen1 halaman2019 System Map COVID-19 Stations FINALwtopwebBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Michael Gerhardt's Opening StatementDokumen10 halamanMichael Gerhardt's Opening StatementStefan BecketBelum ada peringkat
- Loudoun County Teacher Salary PlanDokumen2 halamanLoudoun County Teacher Salary PlanwtopwebBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Gonzales Maryland Poll Report January 2020Dokumen29 halamanGonzales Maryland Poll Report January 2020wtopwebBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Feldman TestimonyDokumen6 halamanFeldman TestimonyGeoffrey Rowland100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- 2020.06.09 Federal Complaint FinalsignedDokumen27 halaman2020.06.09 Federal Complaint Finalsignedwtopweb100% (1)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Pamela Karlan's Opening StatementDokumen6 halamanPamela Karlan's Opening StatementStefan BecketBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Read Turley TestimonyDokumen53 halamanRead Turley Testimonykballuck186% (7)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Catherine Pugh IndictmentDokumen34 halamanCatherine Pugh IndictmentWJZBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Landini MenuDokumen2 halamanLandini MenuwtopwebBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Montgomery County Leaders Urge Board of Education To Study Its Policy On Students Civic EngagementDokumen2 halamanMontgomery County Leaders Urge Board of Education To Study Its Policy On Students Civic EngagementwtopwebBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- BB EnglishDokumen3 halamanBB EnglishwtopwebBelum ada peringkat
- Evidence: Daron Wint's Phone SearchesDokumen19 halamanEvidence: Daron Wint's Phone SearcheswtopwebBelum ada peringkat
- Jack Evans' Attorneys Respond To O'Melveny-Myers ReportDokumen67 halamanJack Evans' Attorneys Respond To O'Melveny-Myers ReportwtopwebBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Chesapeake Bay Crossing StudyDokumen4 halamanChesapeake Bay Crossing StudywtopwebBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Moving Maryland Toward Zero DeathsDokumen18 halamanMoving Maryland Toward Zero DeathswtopwebBelum ada peringkat
- Whistleblower Complaint Against President TrumpDokumen9 halamanWhistleblower Complaint Against President TrumpYahoo News90% (84)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Coal Roasted CarrotsDokumen2 halamanCoal Roasted CarrotswtopwebBelum ada peringkat
- House Republicans Ask Metro For Jack Evans Ethics DocumentsDokumen2 halamanHouse Republicans Ask Metro For Jack Evans Ethics DocumentswtopwebBelum ada peringkat
- Chesapeake Bay Crossing StudyDokumen4 halamanChesapeake Bay Crossing StudywtopwebBelum ada peringkat
- Arthur Capper Senior Apartments Fire LawsuitDokumen28 halamanArthur Capper Senior Apartments Fire LawsuitwtopwebBelum ada peringkat
- Abigail Impact StatementDokumen3 halamanAbigail Impact Statementwtopweb100% (1)
- Katerina Impact StatementDokumen7 halamanKaterina Impact StatementwtopwebBelum ada peringkat
- Daron Wint Cross ExaminationDokumen284 halamanDaron Wint Cross ExaminationwtopwebBelum ada peringkat
- 22 Hours: An American Nightmare - Responses From The ATF LabDokumen2 halaman22 Hours: An American Nightmare - Responses From The ATF LabwtopwebBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Spinach and Feta Cooked Like Saag PaneerDokumen2 halamanSpinach and Feta Cooked Like Saag PaneerwtopwebBelum ada peringkat
- Patient Classification & AssignmentDokumen37 halamanPatient Classification & AssignmentAkhila UsBelum ada peringkat
- Saint Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingDokumen4 halamanSaint Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingimnasBelum ada peringkat
- Perineal Care: Michael H. Esmilla, RN, MANDokumen15 halamanPerineal Care: Michael H. Esmilla, RN, MANHannah Leigh CastilloBelum ada peringkat
- Pathology Integumentary SystemDokumen4 halamanPathology Integumentary SystemMaui GamutanBelum ada peringkat
- Arthritis Fact SheetDokumen2 halamanArthritis Fact SheetClaire MachicaBelum ada peringkat
- Literature Review 1Dokumen5 halamanLiterature Review 1api-582800401Belum ada peringkat
- VEC Question Bank on Biomedical InstrumentationDokumen13 halamanVEC Question Bank on Biomedical InstrumentationNisha ManiBelum ada peringkat
- Indian Kino Tree Bark - VijaysarDokumen3 halamanIndian Kino Tree Bark - VijaysarNeutron ZionBelum ada peringkat
- Annotated Bibliography On Internet AddictionDokumen4 halamanAnnotated Bibliography On Internet AddictionJanet Martel100% (3)
- Appendix 8 PDQ39 PDFDokumen3 halamanAppendix 8 PDQ39 PDFdrrselvarajBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Research Paper DiabetesDokumen8 halamanResearch Paper Diabetesapi-359023534Belum ada peringkat
- 1335 1344Dokumen10 halaman1335 1344Priyanka SharmaBelum ada peringkat
- Abses Perianal JurnalDokumen4 halamanAbses Perianal JurnalAnonymous tDKku2Belum ada peringkat
- 12 OET Sample Referral Letter (Nurse) WritingDokumen43 halaman12 OET Sample Referral Letter (Nurse) WritingAL ' ARIS98% (41)
- Volunteer Report FinalDokumen11 halamanVolunteer Report FinalBeenish JehangirBelum ada peringkat
- Title: Congenital Hypothyroidism: A Ran Sacker Escaping Under The Nose AbstractDokumen6 halamanTitle: Congenital Hypothyroidism: A Ran Sacker Escaping Under The Nose AbstractKavita KhannaBelum ada peringkat
- Autopsy PDFDokumen3 halamanAutopsy PDFstprepsBelum ada peringkat
- Doctors Tell All-And It's Bad - Meghan O'Rourke - The AtlanticDokumen7 halamanDoctors Tell All-And It's Bad - Meghan O'Rourke - The AtlanticAlexBelum ada peringkat
- Reyes Et Al. (2004) - Validation of A Modified Version of The Mini-Mental State Examination (MMSE) in Spanish PDFDokumen11 halamanReyes Et Al. (2004) - Validation of A Modified Version of The Mini-Mental State Examination (MMSE) in Spanish PDFjonas1808Belum ada peringkat
- Biosafety Hazards in the LabDokumen8 halamanBiosafety Hazards in the LabAmalia YusofBelum ada peringkat
- MS Set 1Dokumen6 halamanMS Set 1Julienne ManabatBelum ada peringkat
- College Nursing Exam ReviewDokumen8 halamanCollege Nursing Exam ReviewKenneth NovenoBelum ada peringkat
- Cervical Cancer Literature ReviewDokumen6 halamanCervical Cancer Literature Reviewaflskeqjr100% (1)
- Urinary Catheterization PDFDokumen3 halamanUrinary Catheterization PDFRishabh trivediBelum ada peringkat
- Acute Abdomen During Pregnancy 2014 PDFDokumen584 halamanAcute Abdomen During Pregnancy 2014 PDFlula gestiana taufanBelum ada peringkat
- Primary Progressive Aphasia: Neurological ProgressDokumen8 halamanPrimary Progressive Aphasia: Neurological ProgressDranmar AhmedBelum ada peringkat
- DR Anuj Raj BijukchheDokumen60 halamanDR Anuj Raj BijukchheMUHAMMAD JAWAD HASSANBelum ada peringkat
- Drug Infusions in ICU Made Simple 2016Dokumen28 halamanDrug Infusions in ICU Made Simple 2016ta lê thanhBelum ada peringkat
- (IJCST-V9I3P10:Akshat Rustagi, Rudrangshu Tarafder, J. Rene BeulahDokumen7 halaman(IJCST-V9I3P10:Akshat Rustagi, Rudrangshu Tarafder, J. Rene BeulahEighthSenseGroupBelum ada peringkat
- Fundamentals of hearing impairment and audiological managementDokumen4 halamanFundamentals of hearing impairment and audiological managementsuraj singhBelum ada peringkat
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 3.5 dari 5 bintang3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBelum ada peringkat
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 5 dari 5 bintang5/5 (78)
- Techniques Exercises And Tricks For Memory ImprovementDari EverandTechniques Exercises And Tricks For Memory ImprovementPenilaian: 4.5 dari 5 bintang4.5/5 (40)