Anda mungkin juga menyukai
- Household Environmental Tobacco Smoke and Risks of Asthma, Wheeze and Bronchitic Symptoms Among Children in TaiwanDokumen10 halamanHousehold Environmental Tobacco Smoke and Risks of Asthma, Wheeze and Bronchitic Symptoms Among Children in TaiwanBro IndraBelum ada peringkat
- Maternal Smoking During: and Lower Respiratory Illness inDokumen7 halamanMaternal Smoking During: and Lower Respiratory Illness inshifarahman74Belum ada peringkat
- BBL, Imt, AsmaDokumen7 halamanBBL, Imt, AsmaYenny Adelia 黃梅珠Belum ada peringkat
- BBLR AsmaDokumen6 halamanBBLR AsmaSeptia Pristi RahmahBelum ada peringkat
- Epidemiology On Asthma Human MilkDokumen8 halamanEpidemiology On Asthma Human MilkazaliavirsaBelum ada peringkat
- Jurnal 3Dokumen10 halamanJurnal 3Dian RianiBelum ada peringkat
- The Association of Maternal Age With Birthweight and Gestational Age: A Cross-Cohort ComparisonDokumen10 halamanThe Association of Maternal Age With Birthweight and Gestational Age: A Cross-Cohort ComparisonjoeBelum ada peringkat
- Adult Socioeconmic, Educ. Social Outcome ObesityDokumen6 halamanAdult Socioeconmic, Educ. Social Outcome ObesityMangku Liong GuanBelum ada peringkat
- Risks of Formula Feeding - A Brief Annotated BibliographyDokumen6 halamanRisks of Formula Feeding - A Brief Annotated BibliographyMireiaBelum ada peringkat
- Risks of Formula FeedingDokumen8 halamanRisks of Formula FeedingjpoprockaBelum ada peringkat
- Headache 7Dokumen9 halamanHeadache 7Aden DhenBelum ada peringkat
- Maternal Smoking During Pregnancy Linked to Child OverweightDokumen10 halamanMaternal Smoking During Pregnancy Linked to Child OverweightxquisiteludaBelum ada peringkat
- Prevalence of Asthma in Australian ChildrenDokumen4 halamanPrevalence of Asthma in Australian Childrenoktha_pohanBelum ada peringkat
- A Maternal Vegetarian Diet in Pregnancy Is Associated With HypospadiasDokumen7 halamanA Maternal Vegetarian Diet in Pregnancy Is Associated With HypospadiasancoursBelum ada peringkat
- Pediatrics 2012 Dilley S7 8Dokumen4 halamanPediatrics 2012 Dilley S7 8Elis Sri AlawiyahBelum ada peringkat
- MainDokumen11 halamanMainanita pratiwiBelum ada peringkat
- Nutritional Status of Pre-School Children From Low Income FamiliesDokumen11 halamanNutritional Status of Pre-School Children From Low Income FamiliesFiraz R AkbarBelum ada peringkat
- Kim PholDokumen6 halamanKim PholLiêu VilBelum ada peringkat
- PregnantDokumen10 halamanPregnantm.sandra12340Belum ada peringkat
- Exposure To Environmental Tobacco Smoke and Children Health: Piotr Tutka, Marian Wielosz and Witold ZatońskiDokumen11 halamanExposure To Environmental Tobacco Smoke and Children Health: Piotr Tutka, Marian Wielosz and Witold Zatońskiwawansiswadi01Belum ada peringkat
- Childhood Obesity and Parental Smoking As Risk Factors For Childhood ADHD in Liverpool ChildrenDokumen8 halamanChildhood Obesity and Parental Smoking As Risk Factors For Childhood ADHD in Liverpool ChildrenFabricio CardosoBelum ada peringkat
- Morbilidad Respiratoria en Preterminos FNM 2019Dokumen6 halamanMorbilidad Respiratoria en Preterminos FNM 2019Diana GomezBelum ada peringkat
- Obesity - 2013 - Chen - Prevalence of Obesity Among Children With Chronic ConditionsDokumen4 halamanObesity - 2013 - Chen - Prevalence of Obesity Among Children With Chronic Conditionsmedicinaj021Belum ada peringkat
- Metabolic Syndrome in Spanish AdolescentsDokumen9 halamanMetabolic Syndrome in Spanish AdolescentsSimón JimenezBelum ada peringkat
- Clinical Prediction Rule For RSV Bronchiolitis in Healthy Newborns Prognostic Birth Cohort StudyDokumen9 halamanClinical Prediction Rule For RSV Bronchiolitis in Healthy Newborns Prognostic Birth Cohort StudyJuwita PratiwiBelum ada peringkat
- Alergia e Hipótese Da HigieneDokumen6 halamanAlergia e Hipótese Da HigieneLucas NicolauBelum ada peringkat
- Collier 2006Dokumen7 halamanCollier 2006Adib FraBelum ada peringkat
- Asthma Risk in Children Born After Infertility TreatmentDokumen9 halamanAsthma Risk in Children Born After Infertility TreatmentKinjal ShahBelum ada peringkat
- Philippine Policies On Maternal and Newborn HealthDokumen21 halamanPhilippine Policies On Maternal and Newborn HealthjudemcBelum ada peringkat
- Harju 2018Dokumen9 halamanHarju 2018Habib Budiman AgungBelum ada peringkat
- Sibilancia e PNMDokumen8 halamanSibilancia e PNMPatrícia FernandesBelum ada peringkat
- Microbioma e HiperactividadDokumen9 halamanMicrobioma e HiperactividadMarivi MarinBelum ada peringkat
- Maternal Smoking - NEC MortalityDokumen7 halamanMaternal Smoking - NEC MortalityGlen LazarusBelum ada peringkat
- Sample Research Introduction On Teen PregnancyDokumen12 halamanSample Research Introduction On Teen PregnancyMARY ANGELICA AQUINOBelum ada peringkat
- Impact of Childhood Asthma On Children and Mothers Exploring The Sri Lankan SituationDokumen6 halamanImpact of Childhood Asthma On Children and Mothers Exploring The Sri Lankan SituationInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Gingival Disease in Adolescents Related To Puberal Stages and Nutritional StatusDokumen6 halamanGingival Disease in Adolescents Related To Puberal Stages and Nutritional StatusRosa WeilerBelum ada peringkat
- Folic Acid in Pregnancy: Is There A Link With Childhood Asthma or Wheeze?Dokumen4 halamanFolic Acid in Pregnancy: Is There A Link With Childhood Asthma or Wheeze?Eneydo HgBelum ada peringkat
- Link between youth weight, income and parental BMIDokumen6 halamanLink between youth weight, income and parental BMIq1234werBelum ada peringkat
- Journal Pre-Proof: Clinical Epidemiology and Global HealthDokumen22 halamanJournal Pre-Proof: Clinical Epidemiology and Global HealthClaudia BuheliBelum ada peringkat
- Maternal Risk Factors for HypospadiasDokumen5 halamanMaternal Risk Factors for HypospadiasHamdan Yuwafi NaimBelum ada peringkat
- Asthma JurnalDokumen19 halamanAsthma JurnalZembiland Dwa100% (2)
- PediatríaDokumen8 halamanPediatríaSarahiH.ReyesBelum ada peringkat
- Adolescent Pregnancy Risks and Prevention StrategiesDokumen8 halamanAdolescent Pregnancy Risks and Prevention StrategiesSheylleyBelum ada peringkat
- Family CompotitionDokumen13 halamanFamily Compotitionalif tasya hasani ariaBelum ada peringkat
- Literature of AsthmaDokumen23 halamanLiterature of AsthmaAbrar Hendri PutraBelum ada peringkat
- Jacka. Maternal and Early Postnatal Nutrition and Mental Health of Offspring by Age 5 Years A Prospective Cohort Study Jacka 2013Dokumen10 halamanJacka. Maternal and Early Postnatal Nutrition and Mental Health of Offspring by Age 5 Years A Prospective Cohort Study Jacka 2013sarbu_mirelaBelum ada peringkat
- QoL Obese ChildrenDokumen7 halamanQoL Obese ChildrenLiga Sabatina de BaloncestoBelum ada peringkat
- Origins of Adolescent Obesity and Hypertension: SciencedirectDokumen2 halamanOrigins of Adolescent Obesity and Hypertension: SciencedirectAurnha DewhiBelum ada peringkat
- Jurnal AsmaDokumen11 halamanJurnal AsmaAi Siti Rika FauziahBelum ada peringkat
- Risk Factors for Childhood TuberculosisDokumen5 halamanRisk Factors for Childhood TuberculosisAnthony Huaman MedinaBelum ada peringkat
- Teenege PregnancyDokumen3 halamanTeenege PregnancyJairah LuzBelum ada peringkat
- Risk Factors for Postpartum Depression in Adolescent MothersDokumen6 halamanRisk Factors for Postpartum Depression in Adolescent Mothersdevi maya aristaBelum ada peringkat
- IEHC0049 - Student 13086887Dokumen7 halamanIEHC0049 - Student 13086887virginia.arostegiBelum ada peringkat
- Identification and management of FTT in the communityDokumen5 halamanIdentification and management of FTT in the communityIndri WahyuniBelum ada peringkat
- NIH Public Access: Author ManuscriptDokumen10 halamanNIH Public Access: Author ManuscriptAnnisa RahmaniBelum ada peringkat
- Journal Pone 0252817Dokumen16 halamanJournal Pone 0252817ptriw nigsihBelum ada peringkat
- 1 PB - 2Dokumen6 halaman1 PB - 2Dereje DesalegnBelum ada peringkat
- Childhood Obesity: Causes and Consequences, Prevention and Management.Dari EverandChildhood Obesity: Causes and Consequences, Prevention and Management.Belum ada peringkat
- Obesity and Lung Disease: A Guide to ManagementDari EverandObesity and Lung Disease: A Guide to ManagementAnne E. DixonBelum ada peringkat
- FNBv30n3 Suppl FinalDokumen220 halamanFNBv30n3 Suppl FinalLia Mbag LiaBelum ada peringkat
- Does Antenatal Care Make A Difference To Safe Delivery? A Study in Urban Uttar Pradesh, IndiaDokumen11 halamanDoes Antenatal Care Make A Difference To Safe Delivery? A Study in Urban Uttar Pradesh, IndiaLia Mbag LiaBelum ada peringkat
- NurseDokumen2 halamanNurseLia Mbag LiaBelum ada peringkat
- 22745150Dokumen10 halaman22745150Lia Mbag LiaBelum ada peringkat
- Marinedrugs 10 00727Dokumen17 halamanMarinedrugs 10 00727Lia Mbag LiaBelum ada peringkat
- Kontribusi Asam Folat Dan Kadar Haemoglobin Pada Ibu Hamil Terhadap Pertumbuhan Otak Janin Di Kabupaten Karawang Tahun 2011Dokumen9 halamanKontribusi Asam Folat Dan Kadar Haemoglobin Pada Ibu Hamil Terhadap Pertumbuhan Otak Janin Di Kabupaten Karawang Tahun 2011Lia Mbag LiaBelum ada peringkat
- 22745150Dokumen10 halaman22745150Lia Mbag LiaBelum ada peringkat
- SCABIESDokumen2 halamanSCABIESLia Mbag LiaBelum ada peringkat
- T.catappa Tropical AlmondDokumen20 halamanT.catappa Tropical AlmondLia Mbag LiaBelum ada peringkat
- The Potential of Terminalia CatappaDokumen5 halamanThe Potential of Terminalia CatappaLia Mbag LiaBelum ada peringkat
- Plants That Fight CancerDokumen314 halamanPlants That Fight CancerMai Elnaggar100% (4)
- Assessment of Biological Value of Terminalia Catappa Seed Meal-Based Diet in RatsDokumen7 halamanAssessment of Biological Value of Terminalia Catappa Seed Meal-Based Diet in RatsLia Mbag LiaBelum ada peringkat
- Atra's LectinDokumen6 halamanAtra's LectinLia Mbag LiaBelum ada peringkat
- American College of Gastroenterology GerdDokumen6 halamanAmerican College of Gastroenterology GerdOkki Masitah Syahfitri NasutionBelum ada peringkat
- Cuci TanganDokumen2 halamanCuci TanganLia Mbag LiaBelum ada peringkat
- T.catappa Tropical AlmondDokumen20 halamanT.catappa Tropical AlmondLia Mbag LiaBelum ada peringkat
- Endoscopic Therapies For Gastroesophageal Reflux Disease GerdDokumen17 halamanEndoscopic Therapies For Gastroesophageal Reflux Disease GerdLia Mbag LiaBelum ada peringkat
- Bland Diet For GerdDokumen1 halamanBland Diet For GerdLia Mbag LiaBelum ada peringkat
- Centers of GastroenterologyDokumen8 halamanCenters of GastroenterologyLia Mbag LiaBelum ada peringkat
- Insec's LectinDokumen6 halamanInsec's LectinLia Mbag LiaBelum ada peringkat
- Diagnosing Rhinitis: Allergic vs. Nonallergic: David M. Quillen, M.D., and David B. Feller, M.DDokumen8 halamanDiagnosing Rhinitis: Allergic vs. Nonallergic: David M. Quillen, M.D., and David B. Feller, M.DLia Mbag LiaBelum ada peringkat
- Assessment of Biological Value of Terminalia Catappa Seed Meal-Based Diet in RatsDokumen7 halamanAssessment of Biological Value of Terminalia Catappa Seed Meal-Based Diet in RatsLia Mbag LiaBelum ada peringkat
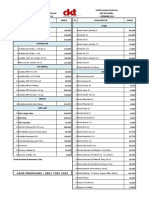
- DKT Indonesia Daftar Harga Produk Kontrasepsi 1 September 2018Dokumen4 halamanDKT Indonesia Daftar Harga Produk Kontrasepsi 1 September 2018YuliantiBelum ada peringkat
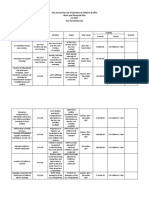
- 2017 CCPC Work and Financial PlanDokumen7 halaman2017 CCPC Work and Financial PlanPatrick Jorge SibayanBelum ada peringkat
- Exam Patient Safety AwarenessDokumen5 halamanExam Patient Safety AwarenessidzniBelum ada peringkat
- Long Quiz Household ServicesDokumen1 halamanLong Quiz Household ServicesJeanne Marie Francisco100% (1)
- Diary Curriculum Map Subject: Mapeh-Health 8 Grade Level: 8 Teacher (S) : Jescil O. Mulit Junior High SchoolDokumen10 halamanDiary Curriculum Map Subject: Mapeh-Health 8 Grade Level: 8 Teacher (S) : Jescil O. Mulit Junior High SchoolJescil Oñez MulitBelum ada peringkat
- The Quarantine War: The Burning of The New York Marine Hospital in 1858Dokumen14 halamanThe Quarantine War: The Burning of The New York Marine Hospital in 1858Patricia DillonBelum ada peringkat
- Ineffective Breast FeedingDokumen5 halamanIneffective Breast Feedingcamilleandaj070575% (12)
- July 2011 Nurse Licensure Examination Result July 2011 Nurse Board Exam ResultDokumen28 halamanJuly 2011 Nurse Licensure Examination Result July 2011 Nurse Board Exam ResultDarren FloresBelum ada peringkat
- Abnormal Labor - ClinicalKeyDokumen32 halamanAbnormal Labor - ClinicalKeyJunior KenBelum ada peringkat
- Primary Health Care QuestionsDokumen7 halamanPrimary Health Care QuestionsAmiel Francisco Reyes89% (19)
- Counselling in HIV/AIDSDokumen34 halamanCounselling in HIV/AIDSBhawna JoshiBelum ada peringkat
- Media Hypes Moderna's COVID Vaccine, Downplays Risks - Children's Health DefenseDokumen10 halamanMedia Hypes Moderna's COVID Vaccine, Downplays Risks - Children's Health DefenseDMDOBelum ada peringkat
- Anti-Rabies Drive Facebook CampaignDokumen12 halamanAnti-Rabies Drive Facebook CampaignMelvin Pogi138Belum ada peringkat
- Clinical Nutrition in Inflammatory Bowel DiseaseDokumen27 halamanClinical Nutrition in Inflammatory Bowel DiseaseJunior Henrique Frey DargasBelum ada peringkat
- Introduction To Microbiology: Dr.B.Reena RajkumariDokumen63 halamanIntroduction To Microbiology: Dr.B.Reena RajkumariSubhi Mishra100% (1)
- Thesis Riza May Ann Leah AutosavedDokumen24 halamanThesis Riza May Ann Leah Autosavedapi-297830299Belum ada peringkat
- Pointers in Mapeh 10Dokumen2 halamanPointers in Mapeh 10HARLEY L. TANBelum ada peringkat
- S1 2022 429533 BibliographyDokumen7 halamanS1 2022 429533 BibliographyNur WahyuniBelum ada peringkat
- Influenza - AiniDokumen11 halamanInfluenza - AiniAl- ImanuddinBelum ada peringkat
- Potential Long-Term Side Effects of Exposure To ChemoDokumen21 halamanPotential Long-Term Side Effects of Exposure To ChemoMichael BubleBelum ada peringkat
- Exercise Prescription For Health & Fittness For Patients With ObesityDokumen1 halamanExercise Prescription For Health & Fittness For Patients With ObesityWasemBhatBelum ada peringkat
- PLMNursing - StudyMaterial - Reproductive PlanningDokumen11 halamanPLMNursing - StudyMaterial - Reproductive PlanningGwyneth ManioBelum ada peringkat
- ScriptDokumen3 halamanScriptPonpimol Odee BongkeawBelum ada peringkat
- Cancer Germany 2015 2016Dokumen158 halamanCancer Germany 2015 2016Sebas ArmasBelum ada peringkat
- ST 3 - Health 6 - Q1Dokumen2 halamanST 3 - Health 6 - Q1Pauline Erika CagampangBelum ada peringkat
- Rujukan: Kempen Cara Hidup Sihat 1997. Kementerian Kesihatan MalaysiaDokumen1 halamanRujukan: Kempen Cara Hidup Sihat 1997. Kementerian Kesihatan MalaysiaArif MuhdBelum ada peringkat
- Menstrual Hygiene Among Adolescent Girls Studying.34Dokumen6 halamanMenstrual Hygiene Among Adolescent Girls Studying.34riniandayaniBelum ada peringkat
- Chicken Pox: BSN 1A Aquino, Cadaoas, Edic, Elegino, Dela Cruz, NepomucenoDokumen20 halamanChicken Pox: BSN 1A Aquino, Cadaoas, Edic, Elegino, Dela Cruz, NepomucenoRayza MaglaqueBelum ada peringkat
- BNSL-043 Block-1 PDFDokumen136 halamanBNSL-043 Block-1 PDFbhoopesh100% (3)
- DM s2022 030dissemination of The Revised School Safety Assessment Tool For The Progressive Expansion of The Face To Face ClassesDokumen15 halamanDM s2022 030dissemination of The Revised School Safety Assessment Tool For The Progressive Expansion of The Face To Face ClassesArgie Corbo BrigolaBelum ada peringkat