Anda mungkin juga menyukai
- Oxygen Therapy in NeonatesDokumen40 halamanOxygen Therapy in Neonatesindiamahesh100% (4)
- Breath ManagementDokumen14 halamanBreath ManagementPaulaRiveroBelum ada peringkat
- NCP Impaired Gas Exchange STROKEDokumen2 halamanNCP Impaired Gas Exchange STROKEMa. Elaine Carla TatingBelum ada peringkat
- CTT CareDokumen76 halamanCTT CareMarites Santos AquinoBelum ada peringkat
- Human Body Systems PPT 2016Dokumen39 halamanHuman Body Systems PPT 2016Jessica Manawes NavorBelum ada peringkat
- Fetal and Neonatal PhysiologyDokumen90 halamanFetal and Neonatal PhysiologyIra Savir100% (5)
- MSDS - CyclohexaneDokumen9 halamanMSDS - Cyclohexanesimbua72Belum ada peringkat
- Science 10 Q4 SLM1Dokumen15 halamanScience 10 Q4 SLM1Zandra Musni Delos Reyes100% (1)
- Principles and Practice of Mechanic (Dokumen1.466 halamanPrinciples and Practice of Mechanic (vvBelum ada peringkat
- Chlorine MSDSDokumen11 halamanChlorine MSDSenviroashBelum ada peringkat
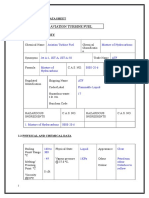
- ANNEXURE-5 Material Safety Data SheetDokumen11 halamanANNEXURE-5 Material Safety Data SheetSuraj KumarBelum ada peringkat
- Postural DrainageDokumen13 halamanPostural DrainageMelisande Rae CiruelaBelum ada peringkat
- Epichlorohydrin Handling and Safety ManualDokumen6 halamanEpichlorohydrin Handling and Safety Manualubaid_nedianBelum ada peringkat
- Ethyl Alcohol Safety Data SheetDokumen6 halamanEthyl Alcohol Safety Data SheetYiannis MinoglouBelum ada peringkat
- Tfacts 124Dokumen2 halamanTfacts 124Jefferson BorgesBelum ada peringkat
- Material Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationDokumen7 halamanMaterial Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationDjordje IvanovicBelum ada peringkat
- Usa Safety Data Sheet: LORD Corporation 111 LORD Drive Cary, NC 27511-7923 USADokumen7 halamanUsa Safety Data Sheet: LORD Corporation 111 LORD Drive Cary, NC 27511-7923 USAErnesto PadillaBelum ada peringkat
- Msds Cuso4Dokumen3 halamanMsds Cuso4Muhammad EvanBelum ada peringkat
- Trikloretilen MSDSDokumen8 halamanTrikloretilen MSDSserhat simsekBelum ada peringkat
- C-9 PlusDokumen6 halamanC-9 PlusArpit MaheshwariBelum ada peringkat
- Chemical Product and Company Identification: Substance: Sulfuric Acid - SpentDokumen8 halamanChemical Product and Company Identification: Substance: Sulfuric Acid - SpentJason DuranBelum ada peringkat
- Acetone CPDokumen6 halamanAcetone CPJonesHutaurukBelum ada peringkat
- Material Safety Data Sheet: Emer Gency O Ver ViewDokumen4 halamanMaterial Safety Data Sheet: Emer Gency O Ver ViewSergio Mendoza ZuñigaBelum ada peringkat
- Material Safety Data Sheet Putri Prilian 195050005Dokumen7 halamanMaterial Safety Data Sheet Putri Prilian 195050005Lulu ArifahBelum ada peringkat
- TCE Solvents MSDDokumen6 halamanTCE Solvents MSDCourtz KrokosBelum ada peringkat
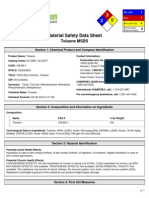
- Material Safety Data Sheet Toluene MSDS Number: M1003 Effective Date: 9/07/2004Dokumen4 halamanMaterial Safety Data Sheet Toluene MSDS Number: M1003 Effective Date: 9/07/2004junglefish71Belum ada peringkat
- Xylene (C H) (CH) CAS 1330-20-7 UN 1307: DescriptionDokumen20 halamanXylene (C H) (CH) CAS 1330-20-7 UN 1307: DescriptionMaris Karisma GintingBelum ada peringkat
- Material Safety Data Sheet: 2-PropanolDokumen3 halamanMaterial Safety Data Sheet: 2-PropanolsalwajodyBelum ada peringkat
- MSDS Rum 60%Dokumen3 halamanMSDS Rum 60%Hugo MarticorenaBelum ada peringkat
- SDS ARC Ethylene Oxide 2013-04-01Dokumen17 halamanSDS ARC Ethylene Oxide 2013-04-01Van SotBelum ada peringkat
- MSDS For Crude GlycerinDokumen8 halamanMSDS For Crude GlycerinGoh AiklengBelum ada peringkat
- Plant Safety: 1. Product IdentificationDokumen8 halamanPlant Safety: 1. Product IdentificationAditya SharmaBelum ada peringkat
- Acrylic Acid MSDSDokumen6 halamanAcrylic Acid MSDSpradeepmenon1982100% (1)
- Material Safety Data Sheet: 1. Product and Company IdentificationDokumen10 halamanMaterial Safety Data Sheet: 1. Product and Company IdentificationFarazBelum ada peringkat
- Ethylene Glycol MSDSDokumen12 halamanEthylene Glycol MSDSAmey ParkarBelum ada peringkat
- Material Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationDokumen3 halamanMaterial Safety Data Sheet: Section 1 - Chemical Product and Company Identificationdalton2003Belum ada peringkat
- Material Safety Data SheetDokumen7 halamanMaterial Safety Data SheetAgnes FerinnaBelum ada peringkat
- Hazardous Substance Fact Sheet: Right To KnowDokumen6 halamanHazardous Substance Fact Sheet: Right To KnowMegh JoshiBelum ada peringkat
- Nital - MSDSDokumen4 halamanNital - MSDSJim2313Belum ada peringkat
- Msds of EdcDokumen13 halamanMsds of EdcMohamed AnwrBelum ada peringkat
- Material Safety Data SheetDokumen5 halamanMaterial Safety Data SheetAni KartibaBelum ada peringkat
- 250 Propoxur-MSDSDokumen2 halaman250 Propoxur-MSDSWuri Handayani EldiBelum ada peringkat
- MSDS Naftalena DafaDokumen8 halamanMSDS Naftalena DafaMuhamad DafaBelum ada peringkat
- ATI-PAO-Safety Data Sheet in Compliance With RegulationDokumen7 halamanATI-PAO-Safety Data Sheet in Compliance With RegulationGochepz Shanz0% (1)
- Material Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationDokumen8 halamanMaterial Safety Data Sheet: Section 1 - Chemical Product and Company IdentificationMunniBhavnaBelum ada peringkat
- Msds - Di Ethylene GlycolDokumen7 halamanMsds - Di Ethylene Glycolsales putrariBelum ada peringkat
- MSDS Amonia LiquidDokumen6 halamanMSDS Amonia LiquidAndrianoBelum ada peringkat
- Safety Data Sheet: Acetone: CHEMTREC: (800) 424-9300Dokumen6 halamanSafety Data Sheet: Acetone: CHEMTREC: (800) 424-9300SACO QCBelum ada peringkat
- Xylene MsdsDokumen11 halamanXylene Msdssheqarayzan0% (1)
- Grotan - MSDSDokumen3 halamanGrotan - MSDSjmquinonesBelum ada peringkat
- Oxalic Acid MSDS: 1. Product IdentificationDokumen4 halamanOxalic Acid MSDS: 1. Product IdentificationhadasadidaBelum ada peringkat
- R 022600Dokumen6 halamanR 022600fructoraBelum ada peringkat
- Isoflurane MsdsDokumen4 halamanIsoflurane Msdsrangga_rspBelum ada peringkat
- TP 125Dokumen141 halamanTP 125Alex SuarezBelum ada peringkat
- Acrylonitrile ICSC: 0092Dokumen6 halamanAcrylonitrile ICSC: 0092Abhishek S PillaiBelum ada peringkat
- Msds TolueneDokumen6 halamanMsds Toluenenirmal_subudhi100% (1)
- Toluene MSDS: Section 1: Chemical Product and Company IdentificationDokumen6 halamanToluene MSDS: Section 1: Chemical Product and Company IdentificationliwirnaberbiBelum ada peringkat
- Sds GluteraldehidoDokumen6 halamanSds GluteraldehidoOchoa Muñoz A QuebecBelum ada peringkat
- Perchloroethylene MSDSDokumen7 halamanPerchloroethylene MSDSWeston DoucetteBelum ada peringkat
- Msds Chloroacetic Acid (Fisher) 1-3-2007Dokumen7 halamanMsds Chloroacetic Acid (Fisher) 1-3-2007witarmayanaBelum ada peringkat
- J.P. Morgan Ventures Energy Corp. New York, NY 10017: 1. Product and Company IdentificationDokumen8 halamanJ.P. Morgan Ventures Energy Corp. New York, NY 10017: 1. Product and Company Identificationbani.vallejosBelum ada peringkat
- Cut Thru MSDSDokumen5 halamanCut Thru MSDSkaylo4613Belum ada peringkat
- CyclohexaneDokumen6 halamanCyclohexaneAnonymous SuC1rG72CBelum ada peringkat
- MSDS - Coolant 50%Dokumen10 halamanMSDS - Coolant 50%Redzwan KadirBelum ada peringkat
- Msds-Calcium Hypochlorite 65%Dokumen7 halamanMsds-Calcium Hypochlorite 65%mhanel edaBelum ada peringkat
- Complementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)Dari EverandComplementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)Belum ada peringkat
- Mmed Anaes A Exam SyllabusDokumen16 halamanMmed Anaes A Exam SyllabusLaserPiratePewPewBelum ada peringkat
- Breathing Techniques-A Review: Subin Solomen, Pravin AaronDokumen5 halamanBreathing Techniques-A Review: Subin Solomen, Pravin AaronekaBelum ada peringkat
- Nursing Care Plans DiagnosisDokumen17 halamanNursing Care Plans DiagnosisSeham AliBelum ada peringkat
- Asthma Davidson + Osmosis + Step Up MedicineDokumen2 halamanAsthma Davidson + Osmosis + Step Up MedicineElyas MehdarBelum ada peringkat
- Lab Manual Week 4Dokumen5 halamanLab Manual Week 4Jonathan SetiawanBelum ada peringkat
- DHF2 CasepediaDokumen2 halamanDHF2 CasepediaKen ZaireBelum ada peringkat
- Paralamento Science Fair 4 BlueDokumen2 halamanParalamento Science Fair 4 BlueMARIA ALEXANDRA POLOBelum ada peringkat
- The Nurse in The Emergency Department Is Caring For A Patient With A PartialDokumen13 halamanThe Nurse in The Emergency Department Is Caring For A Patient With A Partialhasan ahmdBelum ada peringkat
- Death and Its Medico-Legal AspectsDokumen12 halamanDeath and Its Medico-Legal AspectsHarjot SinghBelum ada peringkat
- Grade 9 Quiz 2 LT2Dokumen1 halamanGrade 9 Quiz 2 LT2Ezekiel LapitanBelum ada peringkat
- Biology 2201 - Respiratory System Notes PDFDokumen11 halamanBiology 2201 - Respiratory System Notes PDFVishal SharmaBelum ada peringkat
- Nursing Care With PenumoniaDokumen44 halamanNursing Care With PenumoniaFahmi SyarifBelum ada peringkat
- Birth AsphyxiaDokumen3 halamanBirth AsphyxiaDebjani MukherjeeBelum ada peringkat
- Polysize #5Dokumen4 halamanPolysize #5azambhabibBelum ada peringkat
- Anatomy PresentationDokumen18 halamanAnatomy PresentationZaliaSubplace S5357Belum ada peringkat
- Material Safety Data SheetDokumen2 halamanMaterial Safety Data Sheet123456cc100% (1)
- Homework #2 1. Enumerate and Discuss The 4 Most Difficult Problems Encountered Relating Air Pollution To HealthDokumen2 halamanHomework #2 1. Enumerate and Discuss The 4 Most Difficult Problems Encountered Relating Air Pollution To HealthJonelou CusipagBelum ada peringkat
- German National Guideline For Treating Chronic Respiratory Failure With Invasive and Non-Invasive Ventilation: Revised Edition 2017 - Part 1Dokumen32 halamanGerman National Guideline For Treating Chronic Respiratory Failure With Invasive and Non-Invasive Ventilation: Revised Edition 2017 - Part 1Nafisah Putri WyangsariBelum ada peringkat
- Internalmedicine Sub AnsDokumen90 halamanInternalmedicine Sub AnsSaneesh . SanthoshBelum ada peringkat
- NCP Rds 2Dokumen1 halamanNCP Rds 2Angelokeizer Gavino0% (1)
- Lung Summary LeafletDokumen4 halamanLung Summary LeafletDev Ebenezer JohnsonBelum ada peringkat