Facilitating Informed Decision Making Among Clients of HIV and Sexual and Reproductive Health Services: Literature Review
Diunggah oleh
Jo KaybrynJudul Asli
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Facilitating Informed Decision Making Among Clients of HIV and Sexual and Reproductive Health Services: Literature Review
Diunggah oleh
Jo KaybrynHak Cipta:
Format Tersedia
Facilitating Informed Decision Making: Partner Perspectives
Literature Review
Draft 2
10 June 2009 Plurpol Consulting
Contents
Introduction .................................................................................................................................................. 3 Cordaids perspective ..................................................................................................................................... 4 Changing perceptions of religion and faith in development............................................................................... 6 Sexuality and development ............................................................................................................................ 8 Official Church messages ............................................................................................................................... 9 ... On sexuality and family planning ............................................................................................................ 9 ... On homosexuality ................................................................................................................................ 10 Criticisms of the Church and faith-based organisations .................................................................................. 12 Condoms and HIV/STI prevention ................................................................................................................ 13 The role of conscience ................................................................................................................................. 16 The role of faith in development drawing on faith or doctrine for action ....................................................... 19 Providing sexual health services for young people ......................................................................................... 22 Religious values in a wider context ............................................................................................................... 24 Conclusions ................................................................................................................................................. 28 Annex: Summary of the research methodology ............................................................................................. 30 Annex: Documentation reviewed in this survey ............................................................................................. 32 Annex: Recent statements on condoms by Catholic religious leaders .............................................................. 37
10 June 2009 Plurpol Consulting
Introduction
Discourse on HIV and religion often falls narrowly on the morality and effectiveness of condoms as part of the HIV prevention response. It is important to note that Catholic based responses are wide ranging and include much more than condoms as part of HIV prevention, and cover both treatment and care in addition to prevention. Further, the Catholic response also includes a justice and human rights approach as it examines the broad ranging impacts and underlying causes of HIV. What challenges both HIV and sexual health work is the extent to which cultural and religious ideals about sexuality interact with public health provision. This literature review examined a wide sample of documents which look at the influence of religion on HIV and sexual health service provision. Inevitably the debate on condoms is included, but other issues are of relevance: changing perceptions of religion and faith in development; sexuality in development; official Church messages on sexuality, family planning and homosexuality; criticisms of the Church and faith-based organisations (FBOs); the role of conscience; the role of faith in development drawing on faith or doctrine for action; religious values in a wider context legal, cultural and social; and providing sexual health services to young people. The review concludes with a summary of the issues and importantly which aspects of the impact of faith on HIV prevention and sexual health services are largely missing from current discourse. The annexes consist of the list of documents reviewed and key statements from Catholic religious leaders in support of and in opposition of condoms in HIV prevention.
Background
Cordaid supports Catholic health and HIV/AIDS service organisations in over 15 countries. Many of them are involved in the prevention of HIV and/or education and service delivery concerning family planning and HIV treatment. For most of them the issue of family planning and HIV/AIDS is causing dilemmas as the teachings of the church on sexual morality; conflict with the Catholic social ethics tradition, are not (always) in line with government regulations and not (always) an answer to daily life practices. At the different levels in Church and Church-affiliated organisations, health institutions and AIDS organisations, people address these dilemmas differently. To document this wide spectrum of opinions and approaches (positive and negative) and to highlight some of the key power, gender and influencing factors Cordaid wants to document the practices in this area of its Catholic partners in a few countries. Informed decision making on HIV and sexual and reproductive choices by women and men is probably influenced by religious teachings, policies, structures, and communication styles at all levels of the Church. The literature review focussed on development issues and how they interact with Catholic faith based approaches. This review of currently available literature encompasses a wide range of documents on HIV, sexual health and religious influence in reproductive health. It looks at the impact of development on FBOs and the impact of Church messages on development and FBOs. The review begins with an overview of Cordaids own positions on the issues.
10 June 2009 Plurpol Consulting
Cordaids perspective
Cordaid supports a wide range of reproductive health promotion and HIV prevention programmes in developing countries. Its published and online literature gives little indication that these areas of focus are controversial because of its Catholic faith-based identity, but this does not mean there is no controversy. The values that Cordaid promotes can be found in its reports and speeches: they include justice, solidarity, compassion, and human dignity, among many others.1 Importantly, and perhaps distinct from some other Catholic faith-based agencies, Cordaid not only promotes these values, but also takes a rights-based approach to its work. Its four programme areas (Participation; Emergency Aid and Reconstruction; Health and Well-being; and Entrepreneurship) promote the rights of people to live with dignity and work their way out of poverty.
Controversy
The reason that HIV prevention and reproductive health programmes can be considered controversial for Catholic faith-based agencies is largely because of external expectations placed on them. These expectations are often from Catholic individuals or organisations that may hold similar values, but also base their beliefs on Catholic doctrine. In some cases critics question the validity of Cordaids identification with Catholicism because their work is not perceived to conform to all Catholic doctrine. Arguably this is not possible: Interestingly the most hostile debates on the appropriateness of Cordaids work (and that of other Catholic faith-based agencies) usually take place outside of the development sector. Criticism flows towards Cordaid from conservative Catholic individuals and organisations with information and advocacy roles, rather than organisations working in health and development. In 2005 Cordaid was criticised by several conservative Catholics organisations for supporting the Dutch government's position on reproductive rights as an essential component of strategies to achieve the Millennium Development Goals. For many conservative Catholics the term reproductive rights is a synonym for abortion. In media reports an un-named Cordaid official was quoted as saying: "Participation in reaching these Millennium Development Goals is so crucial that we accept the fact that there may be elements in the statements with which we would deal differently in our practice." (C-FAM 2005) Despite this statement the article was titled 'Catholic' Aid Organization in Holland Supports Plan to Promote Abortion with the word Catholic in inverted commas implying a questioning or derisive attitude towards Cordaids Catholic identity. Critics of Cordaid seem less willing to consider Cordaids promotion of reproductive health where its goal is to reduce the number of abortions (e.g. in Vietnam where the total abortion rate in 1992 was 2.5 abortions per women's reproductive life2) or to prevent forced abortions imposed on girls and women for being unmarried (COS Noord-Holland 2008). But criticism does not flow solely towards Cordaid. In March 2009 Cordaid spoke out unequivocally in contradiction of Pope Benedict XVI when he stated that condoms exacerbate the HIV pandemic. Cordaids press release in response strongly disagree with the Popes statement, reiterated the scientific basis for the role of condoms in the HIV response, and further pointed out that the Popes statement was detrimental to development, and at risk of discouraging and isolating those Catholic health providers that organisations such as Cordaid works with.
Holistic response
Such controversy does not deter Cordaid from promoting a holistic approach to reproductive rights. To narrow the debate to the moral views on abortion is to exclude the broad ranging issues that reproductive health strategies address such as: increasing safe motherhood; reducing the number of unsafe abortions (COS NoordHolland 2008); eliminating female circumcision; promoting alternative to early marriage; and halting forced abortions. Beyond examining the content of these programmes Cordaid also recognise the role of sexual and reproductive health as part of the wider womens rights agenda (Cordaid programme summary, no date).
1 2
Cordaid Directors speech to DRC partners, no date http://www.abc.net.au/rural/worldhealth/papers/35.htm
10 June 2009 Plurpol Consulting
The priority that Cordaid has given to HIV can be seen particularly in its mainstreaming approach and HIV workplace policy approach: partner organisations can apply for grants of up to 2000 (INTRAC 2009) to initiate workplace initiatives including HIV training, organising access to Voluntary Counselling and Testing (VCT) for staff and distribution of condoms. Cordaids portfolio of programmes demonstrates that its commitment to sexual rights: such as its Moldovan project which promotes LBGT3 rights by tackling discrimination, promoting the human rights of minorities and toleration of sexual diversity.4 At the same time, Cordaid clearly articulates an understanding of HIV as a development issue rather than solely a health issue: one that is impacted by gender inequality and stigma.5 It is of course possible to enter into theological and doctrinal debate on these issues. Cordaid does this but usually as an internal exercise within its organisation, among its partners organisations and among Catholic development peers. There seems little point in engaging conservative Catholic critics in debate or dialogue because they do not approve of Cordaids position in which faith plays a passive role according to Clarkes model (see below). Faith is Cordaids motivation for action, religious views are not its output: it provides a development and humanitarian response to people regardless of their religious affiliation and beliefs.
Informed decision making
While Cordaid engages in the debate at times, it does so from a position of commitment to its many partner organisations working where the religious (and social, cultural, legal and political) contexts differ greatly form Cordaids own. This takes us to the heart of the purpose of this research commissioned by Cordaid to understand their partners perspectives on facilitating informed decision making. By commissioning this research, Cordaid moves beyond the top level debates on the hypothetical principles of condoms and abortions, and looks at the realities in which partner programmes operate. Sexual and reproductive health responses require partner organisations to facilitate informed decision making among clients: helping them decide on which family planning and HIV/STI (sexually transmitted infection) prevention strategies are most relevant for them. Cordaid, like any funding agency, has its own set of expectations that it asks of programme partners. This includes providing full and accurate information about all forms of HIV/STI and family planning options, on the basis that it is the role of service providers to support individuals to make informed decisions about what is best for them personally. This may include individuals making decisions in line with their own religious beliefs, but it is the responsibility of the service provider to ensure that all decisions are made with all the information available. In practice this may be easier said than done. Cordaid recognises that there may be challenges to partners, given their own Catholic identities and the other contexts they work in. The purpose of the research is to understand what these challenges are, and how organisations are overcoming them. This includes religious influences, but not in isolation: the legal and cultural contexts will also be considered, and how all three overlap or influence each other.
3 4 5
Lesbian, Bisexual, Transgender & Gay http://www.gay.md/eng/content.php?sid=1 http://www.cordaidpartners.com/rooms/program-8-hiv-and-aids
10 June 2009 Plurpol Consulting
Changing perceptions of religion and faith in development
The interaction between religion (religious leaders, people of faith, and faith-based organisations) and development is steadily being acknowledged and documented as is evident from the approximately one hundred documents reviewed for this literature survey. There is no doubt that a broad spectrum of faith-based agencies, including Catholic, delivers health services including HIV and family planning in developing countries (Parry 2005; FHI 2007). Related to the HIV and sexual health response the following types of response are prominent: Working with young people, orphans and vulnerable children (Drost & Wierda 2006) HIV related treatment including delivering antiretroviral therapy (de Waal 2005; Munro 2005a; Wood 2007) Pastoral care (Phalana 2007) Psychosocial support (Beekman & Beest 2007) Gender issues (Munro 2004; Lambrechts 2007) including gender based violence (EAA 2009) HIV and STI care and support (Munro 2005b) HIV prevention (Munro 2005b) Stigma and discrimination (Insideout Research 2003; EAA 2003)
The scale of the response of faith-based agencies in development to issues such as HIV prevention care and treatment, primary health care and maternal health care is enormous (UNICEF 2005). The World Health Organisation estimates that faith-based agencies provide 25% of HIV services in low-income African countries (WHO 2006) while Catholic faith-based organisations alone are estimated to make up 25-50% of all care for HIV affected people in Africa (NCR 2009). 2560% of the population in 10 African countries rely on just 15 faithbased agencies for drug supplies (WHO 2006). Importantly this recognition of the role of faith-based agencies is increasingly constructive rather than confrontational (Green 2003; Wolfensohn 2004; Tearfund 2006; UNFPA 2004). It reflects a willingness of secular organisations, including governments, donors and NGOs, to engage with faith-based agencies despite, or even because of, the potential challenges (Haddad B, Olivier J, De Gruchy S. 2008) as illustrated by the words of UNFPA Executive Director Thoraya Ahmed Obaid in 2005 reproduced below: Oftentimes, political debates and decisions on these issues have cultural undercurrents that could delay [the] achievement [of MDGs], but other times we find support for change in cultural values and practices and religious interpretations. To make progress, we need to understand these currents. We need to discuss these issues openly. And we need to identify the positive cultural values and religious interpretations which would facilitate moving forward in the promotion of human rights, including the right to reproductive health. Thoraya Ahmed Obaid, Executive Director, UNFPA, 2005 Controversial issues and ideological conflict continue to make headlines but governments, donors, UN agencies and civil society organisations seem to be more willing to engage with faith for several reasons. The strength and reach of faith-based non-governmental organisations have proved themselves to be effective development partners, as evident for example by the funding streams between governments and other donor to FBOs. A fully multi-sectoral response requires the participation of all stakeholders including FBOs. FBOs themselves have formed alliances with organisations based on the same faith, with those of different faiths, and with secular organisations to make themselves heard and to reach out in the spirit of partnership. From the perspective of the policy makers especially at UN level, there seems to be acknowledgement that they need to engage with the issues that perhaps they have previously viewed as problematic if they are to achieve their desired changes. They appeal to the aspects of religion that they view as constructive and open to dialogue and change. UNAIDS explicitly includes active partnership with faith-based agencies (as part of several sectors of society) as one of 12 essential policy actions for HIV prevention (World Association for Sexual Health 2008). The experiences of faith-based multi-sectoral collaboration in secular (Munro 2002; Munro 2005a), ecumenical (Lambrechts 2007) and interfaith (Nubuasah 2006) partnerships have increasingly resulted in the recognition of FBOs as being part of the solution and response to health (Foster 2008; Haddad B, Olivier J, De Gruchy S. 2008).
10 June 2009 Plurpol Consulting
There has also been recognition by Churches that they have been part of the problem (SECAM) and by religious leaders who acknowledge that HIV affects them personally. This is particularly evident from the formation of organisations such as INERELA, the international, interfaith network of religious leaders (both lay and ordained, women and men) living with or personally affected by HIV.
Key research questions
There has been significant increased recognition of the roles and contributions of faith-based agencies in development. The acknowledgement appears to be sincere, and in a genuine attempt to engage faith-based agencies. However, it can be argued that some secular sources view FBOs as an obstacle to public health progress, and this could be one of the motivating factors for the increased attention on them. For those who take this view, an underlying impression is conveyed that (some) FBOs are behind in the development of their responses. The key questions related to this in this research will focus on where partner programmes practice regarding informed decision making fit with changing perceptions by secular organisations of religion and faith in development. How much do stereotypical ideological debates (e.g. condoms vs. abstinence) impact on programme partners perceptions of themselves and their service delivery, especially in relation to facilitating informed decision making? Are the partner programmes responses nuanced and sophisticated enough to demonstrate to external audiences/partners that the faith-based response is are at least as evolved as secular responses?
These questions will be answered based on the sum analysis of the field research tools by the in-country researchers and raised as discussion points in the national workshops with the partners. Whilst the purpose of the research is for Cordaid to understand their partners practice (both strengths and weaknesses) there is also value in sharing key findings with wider audiences, through both faith-based and secular networks.
10 June 2009 Plurpol Consulting
Sexuality and development
It is worth noting that neither the secular or faith-based sectors have a track record of prioritising sexuality in development approaches. Sexuality has typically been addressed by development agencies (secular and faithbased) only in its relation to HIV prevention and birth control, and been regarded as secondary to the important matters of housing, education and employment etc (IDS 2006; IDS 2007). But to fully realise a persons rights, whether they be a minority or not, a response must include their sexual rights (Runeborg 2008; World Association for Sexual Health 2008). Further, sexuality and policy are inextricably linked because the terms for sexual relations are set by policies and politics, including social norms and gender dynamics, national policies and international relations (IDS 2008). In addition, religions (including Christian and Islam) have been perceived to promote the reproductive function of sexuality over pleasure and desire (World Sexual Health Association 2008).
Key research questions
As the literature points out, sexuality and sexual rights are areas which deserve their own prioritisation rather than only being viewed in the context of family planning and HIV prevention. This primary aim of this research is to understand the practices around facilitating informed decision making so it will not focus on sexual rights, but it does provide an opportunity to include data collection on attitudes about sexuality and sexual rights. How do sexual rights feature in partner programmes? Do issues of sexuality and sexual diversity affect the process of facilitating informed decision making?
Staff will be asked how comfortable and knowledgeable they feel in discussing sexuality and sexual-related issues with their clients in the workshop facilitated by the in-country researchers. In addition they will be asked what helps them discuss the issues, and what the barriers are, in order to ascertain good practice, and how CORDAID and its partners can increase their expertise and competence. Staffs raising of sexual issues will also be observed by the in-country facilitators during service provider-client interactions both the range and objectivity of the staffs provision of information. Clients will be asked in the questionnaires and in the focus group discussions how comfortable they feel about discussing sexuality and how skilled they found the partner staff to be. Further questions on their opinions on who is entitled to make decisions on sexual health issues for an individual aim to reveal their attitudes towards sexual rights. The Informed Decision Making conceptual framework (as part of the staff workshop) includes discussion on the delivery of services without discrimination. This will be an opportunity to discuss whether services are provided to people regardless of their age, sexual orientation or marital status. Local or national norms will need to be acknowledged. For example, an organisation may use terminology which implies that it provides services without discrimination but on closer questioning reveal that while they provide services to everyone who is eligible under the law, the law discriminates against unmarried people (as is the case in Indonesia).
10 June 2009 Plurpol Consulting
Official Church messages
... On sexuality and family planning
The most comprehensive encyclical from the Vatican on procreation, and therefore sex and reproduction, is Humanae Vitae issued in 1968. The document issues various directives on the duty of married couples to procreate with marriage. For example, every conjugal act must be open to procreation therefore artificial birth control is unlawful. The ensuing debate centres on two key aspects: whether the encyclical espouses ideals or absolutes; and whether they applicable or relevant to the provision of sexual health and HIV services. Absolute or ideal? The reference to abortion sounds absolute: ...all direct abortion, even for therapeutic reasons, are to be absolutely excluded as lawful means of regulating the number of children. (para 14) But other sections are in less determined language. For example, the encyclical recognises that fidelity can be challenging for individuals but does not expressly forbid it (para 9). The reference to right conscience (para 10) notes that couples have duties to God, themselves, their families and human society. The implication is that the order of priorities is thus. But with right conscience individuals may well change the order or prioritisation in their day to day and lifetime choices and decisions. Conjugal is defined by various dictionaries as of or relating to marriage or the relationship of spouses6 and presumably in this encyclical means vaginal intercourse between a man and a women in marriage. However, this is a narrow definition of sexual expression and with no reference to oral sex, anal sex and non-penetrative sex acts such as mutual masturbation, it is unknown whether these forms of sex are considered unlawful because they are not sexual acts open to procreation or whether they are lawful because they are not mentioned. The gender sensitivity of the encyclicals reflect the time they were written (1960s) as well as the arguably gender-biased nature of Church encyclicals in general. There is inconsistent use of the term man (meaning humankind) with the arguably incorrect pronoun his and interchanged with the use of the term men. Apart from language, one key gender insensitivity is the omission of any reference to the sexual desire of women specifically. With regard to man's innate drives and emotions, responsible parenthood means that man's reason and will must exert control over them. If man in this sentence refers to both men and women, there is no recognition that womens sexual desires are enhanced by their cyclical fertility patterns and their libido is heightened due to increased levels of both oestrogen and testosterone during ovulation.7 Therapeutic means of birth control whose primary function is cure an illness is lawful, however, the text does not include birth control methods whose primary use is prevention. The encyclical associates artificial birth control with marital infidelity and lowering of moral standards (para 17). Another effect that gives cause for alarm is that a man who grows accustomed to the use of contraceptive methods may forget the reverence due to a woman, and, disregarding her physical and emotional equilibrium, reduce her to being a mere instrument for the satisfaction of his own desires, no longer considering her as his partner whom he should surround with care and affection. (para 17)
As mentioned, however, all of the above are moot points when the view is taken that such encyclicals are intended for teaching on contraception not disease prevention (Munro 2005b). At national level, however, these messages are reinforced and explicitly linked to HIV prevention. The Episcopal Conference of Malawi stated that abstinence and fidelity are the only perfect way to prevent HIV. False protection of contraceptives and condoms are listed as a modern ill along with child sexual abuse, incest, rape, widow and widower inheritance, prostitution of street girls and students in secondary schools, colleges, universities and of those in workplaces.
6 7
http://dictionary.reference.com/browse/conjugal http://www.ncbi.nlm.nih.gov/pubmed/15216424
10 June 2009 Plurpol Consulting
... On homosexuality
The Churchs teaching on homosexuality can also cause ambiguity about how Catholic faith-based agencies should respond to sexual health provision. Despite stating that men and women with homosexual tendencies... must be accepted with respect, compassion and sensitivity and every sign of unjust discrimination in their regard should be avoided (Vatican 2003) the language surrounding this statement denotes abnormality and judgement. Preceding the statement on non-discrimination are phrases such as a serious depravity, those who suffer from this anomaly, homosexual acts are intrinsically disordered, and immediately following it are objectively disordered and sins gravely contrary to chastity. The Vatican goes further to say that people who are homosexual do not have the right to marry or adopt children (Vatican 2000) and that non-discrimination against homosexual unions is in fact a form of discrimination against heterosexual marriages. Despite these messages having the potential to incite prejudice, a survey of people from several faiths, including Christians, published by Stonewall (2008) found that although participants acknowledged that some parts of their faith community objected to lesbian and gay sexuality, they felt that these objections were often overemphasised and narrowly reflected by both religious leaders on the one hand and by the media on the other. Furthermore they expressed their support for the rights of gay and lesbian people and for legislation that increases their legal protection. One participant in the survey spoke about the impact of discussing faith with a gay friend and how it changed her attitude: I was certainly bought up to think love the sinner, hate the sin. And it wasnt until... a friend of mine who had told me she was a lesbian, helped me to understand how damaging a statement like that can be. Because if youre saying that, you said you didnt accept her. Because actually you were saying that who she was, was sin within nature, her nature, who she was as a person was sinful. She felt that that totally pushed her away from any opportunity to have faith, she had no right to become part of the Kingdom of God. That really challenged me. The particular survey was conducted in the UK however, and there seems to be little information or research on whether similar views are held by people of faith in African countries.
Key research questions
How do official Church messages on sexuality (including homosexuality) and family planning impact on partner programmes facilitation of informed decision making?
The influence of the Church at all levels is the key subject of the research, and needs to be investigated carefully and sensitively. Staff who interact with clients will be observed during their sessions with clients to ascertain whether they give full information about family planning and HIV prevention services and options. They will also be observed as to whether they raise religious or moral values in the sessions. While this will give us certain data about the sessions, it is important to note that the omission of information and/or the presence of religious references do not automatically tell us there is a negative influence of Church teachings. The raising of moral or religious values, may not necessarily occur in a judgemental or negative manner, while the omission of certain information may be due to factors other than religious influences (e.g. the illegality of abortion may prevent health facilities from providing related information and services). However, recording this data will provide indicators which will allow the researchers to identify any emerging patterns and begin the process of understanding the contexts that the partners are operating in. The heads of the partner organisations will be asked in interviews how their service negotiates the different policy priorities of their stakeholders, which includes the Church, their donors, and the local and national governments. The responses of the partners leadership will be very helpful in analysing the overall context, especially when it is compared to the responses given by the staff during the workshop who will be asked whether they have any challenges in practice in providing a broader range of services than may be perceived as appropriate by interpretations of religious messages.
10
10 June 2009 Plurpol Consulting
In order to understand the context further, the clients will also be asked through the questionnaires and focus group discussions about their own personal religious views, the views of the staff, and how these interact with different options for family planning and HIV prevention. A final review session in the workshop with staff will explicitly invite them to discuss the importance and desirability of separating personal and religious views from service provision. It will also ask them about the influence of hierarchies, be they religious, organisational, donors or government, to understand what external factors have the most impact on their service provision.
11
10 June 2009 Plurpol Consulting
Criticisms of the Church and faith-based organisations
Some observers view the work of the Church as paradoxical; although admired for its leading role in support and care, it receives criticism, and is even considered immoral, for its unwillingness to countenance or even debate condom use (Keough & Marshall 2007). Catholic FBOs also acknowledge this apparent dichotomy (Nubuasah 2006, Munro 2008). In regards to reproductive rights and health, a global survey by UNFPA found beneficial impacts of religion or of religious and cultural NGOs on reproductive health and at the same time, religion was also seen as the most significant barrier to reproductive rights and reproductive health (UNFPA 2005). However, the dichotomous perception belies the variety and complexity of the Catholic faith-based response to HIV and sexual health. It presumes the Church, which articulates cannon law and moral teaching, and faithbased agencies, that deliver health services, make up the same entity or take uniform approaches. In practice, Catholic programmes implement a variety of approaches based on a variety of principles. Furthermore the work of the Church (Keough & Marshall 2007) appears to encompass the activities of the broad array of Catholic faith based organisations regardless of their status: they may base their values on Catholic principles, some receive funding directly from Catholic congregations. Many are professional organisations and registered (in line with national legislation) independent from official Catholic Church funding streams. Other criticisms include: the Church is not AIDS literate enough (Nubuasah 2006); it had a slow start in responding to HIV (Munro 2002); proliferation of ideas such as disease as a punishment from God (EAA 2009); and problems arise due to the hierarchical, male character of some church leadership (EAA 2009). But much of the criticism is levelled at the Church, interestingly not at faith-based organisations, and focuses on its moral teaching on sexuality in relation to STI prevention. It largely comes from secular sources. Among Catholic organisations, those with different views to the official messages, do not often criticize the Churchs hierarchy or messages themselves but offer alternative interpretations of Catholic principles in relation to HIV prevention, and often combined with evidence based public health and human rights messages. Several outspoken Catholic organisations do however take an oppositional stance to the Vatican, for example Catholics for Choice, an advocacy organisation based in the US and largely working in North and South America. Cordaids own messages are very clear that condoms are part (not all) of an appropriate response to HIV prevention.
Key research questions
To what extent do partners work (particularly in the area of facilitating informed decision making) face criticisms directed at: i. ii. The Church? Faith-based agencies?
How do they manage these criticisms?
Much of the discussion around these issues will be addressed in the staff workshop as partners are asked to discuss the external influencing factors on their service deliver, which includes the influence of the Church. Staff will be asked how they manage expectations on them from community members, and other hierarchies (including health policy and legal sectors) which will illicit the kinds of criticisms they face, from where they originate, and how they deal with them.
12
10 June 2009 Plurpol Consulting
Condoms and HIV/STI prevention
Debates about the Church and condoms usually go nowhere constructively because people confuse teaching on contraception with messages about preventing disease. Munro 2005b Both the current Pope and his predecessor both emphasized the prevention approaches of sexual abstinence outside marriage and mutual, life-long fidelity within marriage (Keough & Marshall 2007). A number of times, statements were made which included condoms as not the best or more appropriate solution to reducing HIV infections. For the first time, however, in March 2009 Pope Benedict XVI issued a statement which stated that the distribution of condoms exacerbate the pandemic. A follow up press release was required to clarify the Popes message which played down the negative statement about condoms and reiterated the former arguably ambiguous position on the role of condoms.8 The annex to this review contains examples of statements by Bishops in support of and against condom use in HIV prevention, compiled by Catholics for Choice. The frustration for organisations like Cordaid, is that their message about the role of condoms in HIV prevention is very clear but they are required to reiterate their position to make it clear that they and the Church are not the same entity. Hostile attitudes towards the Church further increase when statements are viewed as scientifically incorrect: for example, Cardinal Trujillos Trujillo claim in 2003 that condoms have tiny holes through which the HIV virus can easily pass (Keough & Marshall 2007). Cordaid and other agencies like them risk reprisals from conservative elements when they issue such counter responses. Conservative vocal members of the Church raise their objections to FBO practices and policies that they view as contrary to Church teachings. For example, the Catholic Action Group launched a campaign9 against the UK based Catholic NGO CAFOD as a result of its publication on HIV prevention in 2004. The media is often quick to highlight issues that it considers divergent or in conflict (example Browder 2007). A polarisation of views has occurred with those for and against condoms each demonising the other side as single issue lobbyists and supporting their stances with arguably partisan experts. A notable example of evidence being used in multiple arguments is the case of Ugandas reduction of HIV prevalence. Uganda famously promoted an ABC approach to prevention and advocates of A and B cite its zero grazing media campaign as the reason for the reduction in prevalence while advocates of condoms cite the increased availability of condoms as the reason. However, this description is an over simplification of the complex context of Uganda. Smith et al (2004) argue that ABC was located, as a key component, among a wider range of risk reduction strategies and contextual factors including: outspoken political leadership by the president and the government; increase in funds for responding to HIV; commitment from public figures including celebrities and religious leaders; rapid provision of both HIV and STI detection and treatment centres; early establishment of care and treatment services; development of local culturally appropriate responses; legislation and cultural changes on practices such as wife inheritance, property rights, ritual scarring; early establishment of multi-sectoral Uganda AIDS Commission; use of interpersonal communication in place or mass media for HIV education; peace and stability after 15 years of war increased employment in both rural and urban areas increased gender equality and legislation to protect womens rights
It is generally agreed that there are several ways to prevent HIV infection or at least reduce risk of infection. Given the variety of individuals circumstances it makes sense that people should be informed of all possible ways of avoiding HIV and STIs so they can make informed decisions about how to reduce their personal risk.
8 9
Unofficial translation by senior Catholic leader on HIV and AIDS 18 March 2009 as of 18/03/09 the website www.catholic-action.com was not functioning
13
10 June 2009 Plurpol Consulting
Theological debates on condom can justify the use of condoms but can also often inadvertently be problematic in themselves. The principle of lesser evil in terms of the motivation for condom use applying to STI protection first, and not contraceptive (Keough & Marshall 2007) is often raised. The difficulty of the discussion getting into the semantics of theological debate is that it can be wholly insensitive towards people living with HIV. A women or a man who is HIV positive and uses condoms chooses this option for the love, safety and protection of their partner, their family and themselves. In the context of upholding dignity and respect for individuals it can be considered unjust to speak about their decisions, and therefore them, in the language of evil and lesser evils. From a human rights perspective, a health response is obliged to include all information about disease prevention and medical treatments to enable individuals to make their own choices. Health promotion is defined by WHO as "the process of enabling people to increase control over their health and its determinants, and thereby improve their health."10 Taking a harder view, it could be said that opponents objections to the policies of FBOs such as Cordaid are irrelevant as these organisations are not in the business of enforcing the moral teachings of the Catholic Church among Catholic clients of services. They work with people from all faiths and none further making it inappropriate to enforce the messages of the Catholic Church. The reality of the interaction between religious messages and health promotion (particularly interventions for most at risk populations) are highlighted by a focus group of men in Kenya who associated condoms with sex workers and inappropriate for church going people (Ambasa, 2002). Equating condoms with transactional sex, extra marital sex and distrust is a prevalent view among communities in both Africa and Asia (Kaybryn 2009). An issue that is currently the subject of much debate is the role of male circumcision in HIV prevention. Muslim members of communities were noted to have lower HIV and STI prevalence rates than the non-Muslims in the same communities. Despite concerns raised by many about the implications for womens health and potential detrimental effects on their already lower negotiation power, control studies were started around the world to test the hypothesis that lower STIs correlated with circumcision. Many of them concluded that within the study period there was enough evidence to demonstrate the hypothesis as valid.11 UNAIDS and WHO agreed that the results of the tests were compelling (WHO/UNAIDS 2007) and began to recommend the inclusion of male circumcision in HIV prevention programmes. Historically the Catholic Church has taken a prohibitive to neutral stance on circumcision in the context of male infant circumcision (Tanner 1990). As far as this literature review has found, there are no recently official church messages on the role of male circumcision in preventing HIV infections. From the perspective of faith-based agencies, some have seen this as an opportunity. Kenyan faith-based hospitals have begun using circumcision, a traditional rite of passage, as an entry point to promote sexual and reproductive health and responsible manhood (de la Torre 2008). However, the promotion of male circumcision is more complex than it would seem at first. A study in 2009 was conducted to understand the role of circumcision for men already living with HIV and their female partners (Lancet 2009). The study was stopped because circumcision of HIV-infected men did not reduce transmission of the virus to uninfected female partners. Further the researchers could not rule out the possibility of higher HIV transmission in couples who resumed intercourse before complete healing of the surgical wound. Many of the studies have focussed narrowly on the data results and not addressed potential questions arising from the promotion of circumcision: Will uncircumcised men be stigmatised? Will circumcised men assume they are invulnerable to HIV/STI infection? Will women make this assumption too? Will male circumcision reduce the negotiation power of women further? Can surgically safe male circumcisions be guaranteed?
Participants at the 6th Global Conference on Health Promotion. The Bangkok Charter for health promotion in a globalized world. Geneva, Switzerland: World Health Organization, 2005 Aug 11. Accessed 2009 Mar 19. 11 For example, see Male circumcision for HIV prevention in young men in Kisumu, Kenya : a randomised controlled trial http://cat.inist.fr/?aModele=afficheN&cpsidt=18528955
10
14
10 June 2009 Plurpol Consulting
Will sex soon after circumcision increase both men and womens susceptibility to STIs if the wound has not fully healed?
As always, no single solution is a panacea for the HIV pandemic and male circumcision may prove to reduce susceptibility of HIV/STI infection in men in the long term as well as the short term but individuals still need to understand all their risk factors and take action accordingly to reduce their vulnerability.
Key research questions
The promotion of condoms within HIV responses and family planning services remains controversial and this research will begin to identify the extent to which partner organisations discuss, provide, or make referrals to clients to access condoms in both HIV/STI prevention and in family planning. The research will identify a much wider range of family planning and HIV/STI prevention options that the organisations provide or make referrals to. How do partners conceptualise the promotion and use of condoms? To what extent are they recommended and distributed as part of i. ii. Family planning services? HIV and STI prevention services?
The observations of the client-service provider interactions will reveal exactly which HIV prevention and family planning options are discussed. The observers check list includes a range of risk reduction approaches to reducing the likelihood of transmission of HIV and STIs. The checklist also identifies which family planning methods are discussed. As a result the research should be able to ascertain whether full and accurate information about all HIV prevention and family planning options are provided. It is problematic to ask clients whether all the options available were offered to them, as they may not have full knowledge of all the options available. However the client questionnaires will ask them whether they were provided with options and choices for either family planning or HIV/STI prevention services during their consultation. The interviews with the heads of the organisations will reveal whether the organisations conform to or reject any policies or messages such as national or global public health standards, CORDAIDs own guidelines or Church teachings.
15
10 June 2009 Plurpol Consulting
The role of conscience
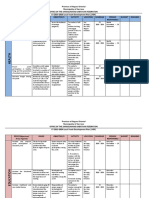
IPPF (2008a) explain in a factsheet outlining the position of the major religions that within Catholicism couples may use artificial, non-abortive methods [of family planning] if they can reconcile using the respective method with their conscience. The role of the individuals conscience receives little mention in recent statements from the Vatican or from most Bishops. However, it is highlighted by participants in a workshop organised by Cordaid in Zambia (2007) who sought to understand HIV and their Catholic identity by reflecting on the stories of Jesus. A very open and honest discussion revealed the participants perceptions of the Churchs achievements and missed opportunities in several areas of HIV prevention. The reference to the conscience is highlighted in the table below, which is reproduced in its entirety because it offer a helpful articulation of the positive and negative consequences of the Churchs messages on the ABC prevention paradigm.
Achievements for the Church High ideals to motivate a high standard Looking at Zambia 85% of the people between 15 and 45 is not infected. Does that mean may be that they abstain? Trust young people to make best choices High self-esteem of young people The fidelity of God is underlining this Its bringing out the essence of being a human being Created confidence and trust Strengthens and stabilises family life Promotes the necessary structure where children can be formed and develop Forms the basis for co-creation: Preventing early orphan hood Christ Church union is as women men union in marriage Reinforced the value of life Preservation of sex for its intended purpose Church has strengthened its clarity on abstinence Mounted high standards Very much in line with the doctrine of Islam Missed opportunities for the Church Media portray sex as something immoral, without human dignity The way the Church has promoted the concept abstinence has been very negative and absolute Abstinence could be formulated as an ideal, not so absolute as it is formulated now Women being infected by the infidelity of their husbands (or the other way around) The Church adopted it so strongly that it lost sensitivity to the problems that can exist between married people Much emphasis on married people. Lost emphasis on faithfulness of non-married individuals Celibate men are making decisions over married people Too hard a rule to be lived Explain fully the sacramental value of faithfulness: It is a channel to holiness Condemned by outside world: seen to be unrealistic Teaching has lost flexibility and has become rigid Lost possibility to mobilize resources Practice of many good people is not in line with what they think/believe the Church is preaching Lost opportunity to live as a living Church; Lost opportunity to dialogue with a number of partners Lost opportunity to widen its stance against the condom (i.e. Discordant couples,.) Failure to help people to form the conscience. (The conscience is supreme!!!!!) Has contributed to the brake-up of marriages) Lost the sensitivity/compassion for the misery of infected people
Abstinence
Fidelity
Condoms
The role of the conscience in North and South America appears to have changed views and practices among people who identify as Catholic. In Bolivia, approximately 70% of married Catholic women have used modern contraceptives at some point, while in Colombia this figure rises to 90% (Harth 2008). Church hierarchy could be said, in Latin America at least, to have more impact on public policy which aligns closely with Church messages, than on its members. In the USA American women of all religious backgrounds believe that access to health care is a right to which all people are entitled and furthermore almost half expected to be able to access all reproductive health options from a Catholic medical institute regardless of Catholic moral laws (Belden Russonello & Stewart 2000) and 60-
16
10 June 2009 Plurpol Consulting
80% of Catholics think that government funded Catholic hospitals should include condoms as part of HIV prevention programmes12 (CFC 2007). In Guatemala, where 75% of people identify as Catholic and 20% are regular church attendees, women may be religious, but when confronted with the realities of life, they often decide to use contraceptives in the interests of their own health and the well-being of their families (UNFPA 2004). A decline in Brazil of Catholic membership is directly attributed to Church attitudes towards contraception (PLANetWIRE 2005). The majority of Catholics believe that condoms are pro-life13 (CFC 2007). But among African and Asian communities there is less evidence that people who identify as Catholic have similar views on contraception, sexual health provision and condom use which are independent of Church messages. The participants in the Cordaid Zambia workshop, however, were very clear about what messages the Church should promote in regard to condoms: Rather than only condemning the condom it is about protecting life and the beauty of sexuality. Protect the goodness of sexuality and protect life; Recognize that the condom is a element but only one element in the solution ( Church to acknowledge this) Stress the importance of informed decision-making by offering options to people involved The Church to expand the teaching of the supremacy of individual conscience on the use of condoms in the context of marriage in line with the principle of subsidiarity Attention to be drawn to the principle of double effect; The Church to take the responsibility for an opening of the use of condoms in the context of marriage.
Reflecting on the Vaticans current actions and statements in relation to sexual and reproductive health, it is worth considering (and developing) the following analysis of its Strengths, Weaknesses, Opportunities and Threats: Strengths Values which promote human dignity, compassion, justice and love Providing ideals for Catholic individuals to aspire to Faith in action as demonstrated by the faith-based response Weakness Attempts to apply doctrine designed for the individual conscience to public health situations The doctrine in totality is contradictory (e.g. can one promote human dignity and compassion for the poor while forbidding contraception at the same time?) Some doctrines promote the non-acceptance of people who are homosexual Opportunities Framing constructive, inclusive and participatory values to motivate action Move beyond the condom/abortion debates in sexual and reproductive health and focus on building the capacity of the individual to exercise their conscience. Develop theological positions about the moral imperatives for access to services for all Threats Application of the moral framework for individual decision making to public health issues undermines the Churchs credibility with both Catholic and secular organisations Increased gender inequality due to the Churchs lack of promotion of womens rights Increased risk of STIs (including HIV) due to denial of the role of condoms in the HIV response
12 13
Ghana: 60%; Ireland: 87%; Mexico: 86%; Philippines: 65%; USA: 73%. Source CFC survey 2007 Ghana: 59%; Ireland: 86%; Mexico: 90%; Philippines: 77%; USA: 79%. Source CFC survey 2007
17
10 June 2009 Plurpol Consulting
In Western industrialised countries, there is little discussion on the role of conscience because, anecdotally, it is taken for granted, as evidenced by the fact that so many individuals fulfil behaviours that are at odds with Catholic doctrine and still identify themselves as Catholic: including using contraception, undergoing abortions, getting divorced, exercising homosexuality, having pre- and extra- marital sex etc. The level of autonomy that European, North and South Americans Catholics exhibit, appears to be much higher than many Catholics in developing countries. The SWOT analysis above can be developed considerably and the national workshops with partners may provide an ideal opportunity to consult the partners programmes on their perspectives.
Key research questions
The role of the conscience of the individual is an important, yet under stated part of Church messages and reproductive health. While partner organisations will not be expected to take a theological approach to supporting individuals develop the role of their conscience, they will be expected to take a public health approach to helping clients make informed decisions. In this regard it will be interesting to see how the partner organisations reconcile all combine the theological and public health approaches, if at all. How does the role of the clients conscience feature in the process of facilitating informed decision making? How do partner staff understand the role of their own conscience as part of providing objective service provision?
The observations of the client-service provider interactions will note the behaviour of staff in helping clients make informed decisions, and whether they raise their own or the clients religious or personal views in the process. The conceptual framework on informed decision-making as part of the staff workshop provides an opportunity for staff to discuss all of the key issues around facilitating the process. This includes the legal, practical, financial, organisational, community, national and religious influences that both facilitate and hinder the process. The final review session with staff in the workshop explicitly raises the issue of whether it is desirable and necessary to separate personal and religious views from the provision of services. The self-assessment tool identifies the organisations own perceptions of where their strengths are in the five key elements of facilitating informed decision-making: for each of the five elements (A: service options are available; B: the decision-making process is voluntary; C: individuals have appropriate information; D: good client-provider interaction; E: the social, religious and right context support autonomous decision-making) the partners will be asked to decide from five levels where their current strengths are. The five levels are: Level 1: indicators that shows we are aware Level 2: we act within constraints Level 3: we aim for a holistic approach Level 4: continuous action, systemising what we do Level 5: the practice as part of our lifestyle
18
10 June 2009 Plurpol Consulting
The role of faith in development drawing on faith or doctrine for action
But while Church encyclicals provide the official teaching position of the Church on certain issues, other documents provide guidance on the appropriate action for responding to development situations, including the response to HIV. The SECAM Plan of Action (2002) reaffirmed the UNGASS commitments on treatment and prevention of HIV and committed to action in six areas: advocacy; stigma and discrimination; partnership/ collaboration; care and prevention; resources; and gender. The section on Care and Prevention includes two actions related to sexuality: Develop curriculum that integrates HIV/AIDS into theological and religious education particularly on issues related to its social effects, discrimination and stigma and that strengthens moral education on healthy relationships and sexual integrity in the context of HIV/AIDS. As leaders, come up with concrete programmes that focus on sexual health education, behavioural change, HIV/AIDS counselling in order to link prevention with care and support The tone of the document is of recognition of the contribution of faith-based organisations and a call to action. It is the underlying values of faith that FBOs themselves are keen to return to and to promote in their efforts to respond to the realities of development: compassion, justice, human dignity (Phalana 2007; Masimba 2008; EAA 2009), alleviating suffering (Pearson 2007), solidarity and the common good (EAA 2009), and subsidiarity (van Beuningan 2006). Recent statements from the Vatican have also appealed to Christian values to respond to HIV rather than doctrine to determine action (Vatican World AIDS Day Statement 2007). Clarke (2005) distinguishes between four main ways in which FBOs deploy their faith through social or political engagement or link faith to developmental or humanitarian objectives:
Passive Faith is subsidiary to broader humanitarian principles as a motivation for action and in mobilising staff and supporters and plays a secondary role in identifying, helping or working with beneficiaries and partners.
Active Faith provides an important and explicit motivation for action and in mobilising staff and supporters. It plays a direct role in identifying, helping or working with beneficiaries and partners, although there is no discrimination against nonbelievers and the organisation supports multi-faith cooperation.
Persuasive Faith provides an important and explicit motivation for action and in mobilising staff and supporters. Plays a significant role in identifying, helping or working with beneficiaries and partners and provides the dominant basis for engagement. Aims to bring new converts to the faith or to advance the faith at the expense of others;
Exclusive Faith provides the principal or overriding motivation for action and in mobilising staff and supporters. It provides the principal or sole consideration in identifying beneficiaries. Social and political engagement is rooted in the faith and is often militant or violent and directed against one or more rival faiths.
A challenge for understanding FBOs is that their approaches can vary within these distinctions. For example, donors currently tend to favour passive and active FBOs as their faith motivates their response without proselytisation or without the promotion of one faith to the exclusion of others. However, the policies and practices of an FBO may be passive or active on one issue yet persuasive or exclusive on another. Here Clarke specifically references the example of the Catholic Church which can be dogmatic on issues such as sexual and reproductive rights and HIV/AIDS prevention, yet supportive of other aspects of development discourse and policy. Through this statement, however, Clarke inextricably links the official Church with the responses of the Catholic FBOs. And as CAFO point out "We do not teach dogmas; we teach skills," (CAFO 2007).
19
10 June 2009 Plurpol Consulting
The messages of the Church that FBOs draw on to motivate their response include compassion and nonjudgement (UNFPA 2004). For example, in a speech to DRC partners, Cordaids director draws on the actions of Jesus rather than the doctrine of the Church. In reference to the story of Jesus treatment of the women accused of adultery, Jesus does not set himself up to judge or condemn, but to change. Jesus wants her to change but that she has to do by herself and therefore it is apparently not so relevant to judge. (Cordaid no date) The very basis of the purpose of spirituality is discussed by Bishop Kevin Dowling: Spirituality can have more than one purpose. But in terms of our topic, I think one important factor in peoples lives is the need to understand their own situation now and make sense of it. Central to all this is the perception that HIV/Aids is caused by immoral behaviour which could be understood in terms of a Christian morality, or other forms of morality, e.g. African morality systems. That notion of being infected because of immoral behaviour needs to be dealt with, or rather responded to only in the light of how Jesus related to the outcasts and the so-called sinners in the Gospel and not in terms of any other understanding of morality. Jesus simply asked us not to judge never. (Dowling) There are many examples of resources for drawing on Christian doctrine for reflection (Speicher and Wilson 2007) and for discussing the negative impacts of Christian message and how to approach these such as reading the bible critically (Paterson 2005), and working with religious leaders (UNICEF 2003; Burket 2006). Muslim FBOs face a range of challenges in a similar context to that of Christians, namely criticism aimed at the religious leadership including being slow to act to the HIV pandemic and denial of the existence of behaviours among the Muslim population which increase risk to HIV and other STIs (NBR 2005). But examples of successful interventions, particularly the identification of local religious leadership as key conduits for information, are increasingly being documented (UNAIDS 1998). Several publications support theological reflection on HIV prevention, care and treatment in relation to Islamic teaching and values (Positive Muslims 2004 & 2007) and reach out to Muslim leaders to respond to both HIV prevention and reproductive health (USAID 2007). Womens rights groups in Muslim societies have embraced the challenges of confronting and realising sexual rights in the contest of patriarchal control over womens sexuality (WWHR website). Many Muslims interpret Islam doctrine in relation to contraception in a way that permits contraception for married couples (pre- and extra-marital sex is forbidden under Islamic law). The Prophet exclaims to his people to marry and procreate in the Quran which places marriage in the context of not only sexual gratification but also of parenthood.14 At the same time, concurrent messages about Allahs desires for his people promote a sense of making the timing and spacing of children important so that parents are able to be the best parents they can be. This includes avoiding having children if meeting their needs will bring hardship on the family. According to Islamic Reliefs website, abortion is allowed up to 120 days into the pregnancy if the lives of either the mother or child are endangered by the pregnancy.15 The other two reasons abortions are permitted under Islamic law are: the pregnancy has occurred as a result of rape, and if the child is likely to be severely disabled. On the basis of reducing vulnerability (poverty and HIV infection) and the fact that many peoples realities do not conform to Islamic laws ideals, family planning and HIV prevention (including the use of condoms) are accepted as necessary parts of the development response by organisations such as Islamic Relief.
Key research questions
In terms of identifying the ways that the partner organisations deploy their faith through their service provision, Clarkes model of Passive, Active, Persuasive and Exclusive engagement is not nuanced enough for the purpose of this research. The research assumes that they organisations are motivated by their faith, as they identify as Catholic-based. In Clarke's model they are likely to be categorised as passive or active. However, within the daily practice of the organisation we want to know what influence church doctrine has on action.
14 15
To what extent do partners draw their motivation for action from faith or doctrine? How does motivation from faith and/or doctrine interact with public health policy?
IslamOnline.net discussion forum http://www.islamic-relief.com/Indepth/reprohealth.aspx
20
10 June 2009 Plurpol Consulting
Is it possible to place partner programme responses (or aspects of their services) in relation to informed decision making within Clarkes model: passive/active/persuasive/exclusive? Can Clarkes model be further refined to describe the attributes of the partners programmes?
The observation of staff-client interaction will reveal whether religious views are raised in consultations, and whether the spare parts in facilitating me informed decision-making process. However these observations will not reveal whether the impact is negative or positive. So the observations will also monitor whether the staff appear to guide clients decisions. The final review session with staff as part of the workshop will specifically ask what the influences from higher hierarchies. This includes influences from within the organisation, the Church, the donor and the government. In relation to the Church, it will be interesting to see explicitly what those influences are, and whether they originate from local, national or Vatican sources. The interviews with the heads of the organisations also explicitly raised the issue of influence of external influences on service provision, including expectations from church leaders. In addition the interviews will include questions on whether the official messages from the Vatican on condom is part of the HIV response and artificial contraception within family planning effects their organisations Provision of services. The interviews will also seek to understand what the enabling and limiting factors of the organisation's catholic identity are in facilitating informed decision-making. Throughout the field of search the in country researchers will observe and note the extent to which faith and doctrine play a part in the partner organisations provision of services.
21
10 June 2009 Plurpol Consulting
Providing sexual health services for young people
If sexuality as a right is a challenge to all development actors, both faith-based and secular, then sexuality and young people is even more difficult to approach. Sex and sexuality are widely regarded as taboo, especially where adolescents are concerned; this taboo is a constraint to adolescent reproductive health (UNFPA 2005) and continue to persist (Munro 2003). There are laws in place in many countries which prohibit family planning services to young people or those who are unmarried (e.g. in Indonesia). The debate around whether sexual health information is appropriate to provide to young people still goes on in many faith and secular contexts despite evidence to show that fully informing young people gives them the opportunity to understand the impact of behaviours and decisions on themselves. In fact, those who have full information are more likely to be risk-averse than those without (Christian Aid 2003; UNFPA 2002). Sexual health and HIV education, including related life-skills education neither hasten sexual debut nor increases the number of sexual partners. Hence sex and HIV education does not promote promiscuity amongst young people.16 Furthermore, good quality sexual health and HIV education both reduces levels of pregnancy and STIs, including HIV and reduces stigma and discrimination against people living with HIV and AIDS. It is clear from a number of studies that young people including those who identify with a faith are sexually active and engage in vaginal, oral and/or anal sex (Fikelela AIDS Project, 2005). There exists a gap between the Churchs traditional teaching of no sex before marriage and the realities of the way in which our young people live. Is the message of abstinence not reaching these young people, or is it ignored? Either way the authors of the Fikelela report acknowledge the reality of the behaviour of young people: we should no longer hide our heads in the sand and pretend that our young people are not at risk. The National Childrens Bureau in the UK takes a rights-based approach: young people (including those of faith) are entitled to sex and relationships education that is relevant to them (National Childrens Bureau 2004). A number of publications aimed at young people address sexuality from a Christian perspective alongside issues like identity, values, healthy relationships, biological changes, communication, making decisions, saying no to sex, pregnancy prevention, STIs, family, responsibility, safety, and respect (FHI 2006a; 2006b; 2006c). Similar guides are available for working with young people from a Muslim perspective (FHI 2006d). There remain many challenges for both young people and those who work with them. The observations of Kelly (2003) are still relevant today. Young people are deterred from accessing testing and health services for several reasons: services are often not youth-friendly meaning they are not aimed at young people and therefore do not cater for their needs. Anecdotal evidence even describes services that actively deter young people. Sometimes this is due to the personal attitudes of individual staff members who have no training in working with young people, and sometimes the legal framework prohibits sexual health services to minors or unmarried people (as in the case of Indonesia). As a result young people may be afraid to access existing services, and coupled with anxiety or embarrassment about sexuality, overall there is little incentive to know their status or seek help and information. Even when young people have knowledge about how to prevent STIs there are particular barriers to using condoms. Kelly cites the association of condoms with implying a lack of trust in ones partner. The influence of peers can have negative and positive impacts on young people and can increase or decrease their sexual activity or take the precautions to reduce their risks of HIV/STI infection and pregnancy. Gender inequality puts young women and girls at risk because they are less likely to be able to negotiate sexual encounters. Young people are also at risk of domestic abuse, coercive sex and sexual violence. Kelly notes the societal double standards for sexual and other behaviour which prevail for men and women, and for older and younger people. Evidence from the focus-group discussions indicates that adolescents are aware of the conflict between choice of strategy (abstinence and condom use) and sometimes conceal their condom use in order not to disappoint adults. In some cases, their moral conflict gives young people limited choices about reproductive behaviour (Population Council 2003).
16
Christian Aid 2003
22
10 June 2009 Plurpol Consulting
Key research questions
The research provides an opportunity through limited data collection to observe whether different types of information are provided to clients of different ages and gender. While a comprehensive analysis of the ages, sex and marital status of all clients attending any of the health facilities is not possible, we will be able ascertain a certain amount of information about selected clients through the questionnaires, and through observing the client-service provider interaction. However, we may find a bias in the profile of clients who complete the questionnaires and who consent to having their session observed, for example, if there is a correlation with young people and a lack of confidence in discussing their visit, then fewer young people are likely to participate in the research. Attitudes towards young peoples sexuality and whether services are provided to youth and unmarried people will be sought through the research which will seek to answer the following questions: Which partner programmes provide HIV prevention and family planning services to young people? How do attitudes towards young peoples sexuality impact on the service provision and facilitating informed decision making among them?
In order to understand general attitudes towards young people, a question in the client questionnaire will ask clients who services should be available for (including adolescents and unmarried people) and who should make decisions about family planning and HIV prevention. Staff attitudes towards young people will also be examined in the staff workshop, particularly the session which discusses whether The social and rights context support autonomous decision making. This section takes a broader view and asks whether laws, policies and social norms support gender equality, peoples right to make decisions for themselves, and whether services are provided regardless of clients age, sex, marital status and sexual orientation.
23
10 June 2009 Plurpol Consulting
Religious values in a wider context
The messages from the encyclicals and the many Bishops who apply Church teaching on marriage and sexuality that usually forms opinions about the Church by its members and observers, and that become inextricably linked to faith based agencies working in health and development. Just as the policy of a government reflects on the citizens, so does the policy of the Vatican reflect on the Churchs members, and in both cases there is rarely uniform support or adherence to the edicts issued. The Church provides moral law not public health messages. The complexity for many individuals is that their societal beliefs consist of many elements, not only religious. The cultural, legal and personal all interact with the religious (see diagram below). All of these aspects have varying influences at different times of peoples lives and on different aspects and are subject to change as priorities and circumstances change. This poses interesting questions for faith-based agencies working on development and health issues. What part of their work is based on their faith the impetus for action, the selection of staff and partner organisations to participate in the work, the design and implementation of programmes? And are the aspects of faith which inform the response selective by necessity as not all doctrine is directly relevant to the theme of the work and combined with other approaches such as rights-based and public health approaches? For example, there are many cultural practices (some linked to religion, some not) that have posed threats to sexual health. A UNFPA survey reported that people (from African and some Asian countries) cited various practices associated with marriage as constraints to achieving sexual and reproductive health and rights (UNFPA 2005). These included early marriage (Africa and Asia), polygamy (Africa), and widow inheritance (Africa and Asia), all of which contribute to the transmission of HIV and other reproductive health problems. Female genital mutilation/cutting is detrimental to the health of girls as well as a violation of their rights. Countries in Africa and some Arab States indicated that the practice is a serious constraint to progress in gender and reproductive health. The legal framework can also pose challenges, for example, the illegality of homosexuality or abortions. There is also myriad of international commitments and conventions government must, in theory, abide by or aim for (see box: International Commitments). Religious, cultural and legal influences are also part of an even wider more complex picture of the epidemic and the context in which HIV and sexual health services are provided. On the HIV Problem Tree (see page 27), we can see these issues reflected in the roots of the causes of HIV. The first layer (sex-blood-mother-to-child) shows the biological roots of transmission. Further biological drivers of the epidemic include the presence of other sexually transmitted infection, pregnancy or an immature or injured genital tract, times of high viral load such as after acquisition of the virus (EAA 2009). The next two layers (political/economic migration sexual violence - sex work/bartering ignorance stigma peer/social pressure unemployment poverty substance abuse) highlight factors that increase individuals vulnerability to HIV transmission. These imply behavioural drivers of HIV transmission and also include unprotected sex or multiple sexual partners, intergenerational sex, early marriage or early sexual first sexual experience, injecting drug use, violence against women or children, and indirectly alcohol and drug use which can increase risk taking behaviours (EAA 2009). The final two layers (war legal political religion/culture trade poverty (local and North/South) gender inequity) highlight the structural and contextual factors that increase vulnerability to HIV transmission. This research is most concerned with the legal, religious and cultural contexts and how they impact on health service providers. Religious and cultural drivers of the epidemic include existence or reinforcement of taboos around
24
10 June 2009 Plurpol Consulting
discussing sex, exacerbated among adults working with young people, understandings of disease linked to sin and punishment from God (EAA 2009) resulting in stigma and discrimination, particular positions on HIV prevention approaches a described above, and practices that place people at particular risk of HIV transmission such as wife inheritance, inter-generational sex, cleansing ceremonies, female genital mutilation (EAA 2009). What the problem tree demonstrates is that [aspects of] religion can be a driver of the epidemic in the sense that it creates conditions which exacerbate HIV transmission. The Problem Tree challenges us to look critically at all the contextual factors that increase individuals International commitments susceptibility to HIV transmission, including (and not exclusively) the relevant aspects of religion. The increased recognition of the role of faithbased agencies in the response to HIV and increased dialogue between FBOs and secular actors, research on the impact of religion and culture has focused on the individuals in communities their religiosity and behaviour and attitudes. However, much less research has taken place which focuses on the challenges of individuals and agencies who provide services, and whether they approach HIV and sexual health by addressing the biological, behavioural and cultural drivers of the STIs and the contexts in which they implement their actions: the legal, religious and cultural contexts. Several studies have attempted to identify whether faith or rather religiosity impact positively on the behaviour of individuals in terms of reducing their risk to HIV and STIs (Regenerus & Trinitapolis 2006; Trinitapolis 2006). The results were somewhat ambiguous as it is difficult to discern whether self-reported information about behaviour and perceived risk of infection are reliable. For example, the reasons that individuals were more likely abstain from extra marital sex are not necessarily attributable to their religiosity and could be equally due to local cultural values. Similarly, individuals who attend services regularly were found to report higher likelihood of present or future HIV infection than less regular attendance, and this could be attributed to their increased awareness of HIV exposure through messages received via their church rather than practising high risk behaviours. But a wide variety of factors impact on peoples behaviour and decision making. For example, womens [decision or ability to] access to maternal health care depends on: place of residence; socioeconomic status; age; ethnicity; education; religion; culture; clinical need for care; decision making power; costs, location and quality of health services (Say and Raine 2007).
...on Development UN Millennium Declaration (Millennium Development Goals) 2000 UN World Summit (Millennium Review) (2005) ...on Human Rights including Womens Rights Universal Declaration of Human Rights, 1948 Beijing Declaration 1995 CEDAW 2003
...on Reproductive Health Plan of Action, International Conference on Population & Development, UNFPA, Cairo 2004 Ottawa Commitment 2002: 2002 International Parliamentarians' Conference on the implementation of the Programme of Action of the International Conference on Population and Development (ICPD) Strasbourg Commitment 2004: International parliamentarians affirmation of Ottawa 2002 and Cairo 2004 World Population Plan of Action, World Conference on Population 1974 Maputo Plan of Action on Sexual and Reproductive Health and Rights, 2007-2010. Special Session of the African Union Conference of Ministers of Health entitled Universal Access to Comprehensive Sexual and Reproductive Health Services in Africa. Maputo, 18-22 September 2006. Continental Policy Framework on Sexual and Reproductive Health and Rights. Adopted at the 2nd Ordinary Session of the Conference of African Ministers of Health, Gaborone, 10-14 October, 2005 ...on HIV and AIDS Abuja Declaration on HIV AND AIDS, Tuberculosis and other related Diseases (2001 and 2007) African Union, HIV, Malaria, and TB Health Strategy (2006) UNGASS Political Declaration (2001 and 2006) Lom Declaration on HIV AND AIDS in Africa (2000) Universal Access to HIV Prevention, Care and Treatment by 2010 (2005) ...on Health African Union Africa Health Strategy (2007-2015) calls for family planning to be framed in broader reproductive health services in a comprehensive approach to womens sexual rights
25
10 June 2009 Plurpol Consulting
In terms of accessing reproductive health & commodities a significant barrier to people of all ages is the actual supply of commodities (invasive birth control etc) and the necessary accompanying surgical equipment (IPPF 2008b). The reasons for supply deficiency include: Financial gaps that have to be closed by the international donor community political barriers such as tariffs, taxes, and international registration mechanisms external restraints as regards the purchase of cost intensive medication through pharmaceutical companies and exporting countries, and other trade restrictions international laws such as patent rights insufficient, ineffective or inadequate logistic systems inefficient supply channels and supply chain management lacking technical and human resources inefficient coordination of the stakeholders lacking quality control of the counselling offered
From a theological perspective, different values and norms may be applied to the macro and micro level. As shown by the Church in Latin America, it is possible to be very effective at the macro level in terms of promoting justice issues and concepts such as solidarity and partnership. These can, of course, be translated into action at community and service delivery levels. In addition, the values of compassion and human dignity have very immediate applications in human relationships, which extends to interactions between service providers and their clients.
Key research questions
The research will seek to understand the complexity of the environments that the partner organisations are operating, and whether there are conflicting expectations in terms of public health, legal and religious paradigms. At the same time the research will also aim to identify good practice where organisations are able to successfully combine views to provide a holistic service. Based on the model above which proposes that three major influences (legal, religious, cultural) impact on the individual, the research will seek to answer the following questions: What are the contextual factors on partner programmes that impact on the programme in general and facilitating informed decision making in particular? How significant are religious influences are they more or less compared with legal and cultural factors and how possible is it to distinguish between the three proposed influencing factors? If the influencing factors are distinguishable, do they compete with each other (causing conflict) or do partners find ways to promote their compatibility?
Observation of the working environments of the partner staff will identify any challenges in terms of difficult or under resourced facilities, which may in turn contribute to lower levels of support provided to clients to make informed decisions.
The personal and professional views of the staff will be sought through the workshop with partners, in order to hear from them first hand whether they feel any conflicting pressures. The observed interactions between staff and clients will verify how staff behave, and respond to their clients views. Clients reflections on the services provided and whether their own personal/religious views about family planning and HIV prevention services will be sought through the client questionnaires and focus group discussions in order to increase our understanding of the context that the partner organisations work in.
26
10 June 2009 Plurpol Consulting
27
10 June 2009 Plurpol Consulting
Conclusions
There has been a noticeable change in the perception of the role of faith-based responses by secular sectors, which has moved from a position of non-engagement to constructive dialogue. In many ways the debate around how faith-based agencies approach sexuality is over-emphasised in relation to the very significant lack of response by secular agencies. Both secular and faith-based agencies are particularly challenged by cultural and/or legal contexts to working with young people on sexual health. Official Church messages focus on the context of marriage and contraception and are arguably applied inappropriately to disease prevention and public health service provision. Praise for the Churchs response to HIV assumes little or no distinction between the Church itself as a religious institution and the responses of hundreds of faith-based agencies. The Church response is therefore viewed as contradictory when juxtaposed with the official Church messages. In reality, most faith-based agencies draw on their faith principles to inspire action rather than Church doctrine. The role of the conscience in Catholicism is rarely highlighted by the Church or Bishops in communications about HIV prevention, and often neither by faith-based agencies engaged in the debate on the use of condoms. The religious values of individuals are part of a much broader context, as is the impact of religion on HIV transmission. Perhaps what is more interesting is the information that this literature review was unable to find: while the impact of religion on individuals is well documented, the competing demands on health workers actually providing services receives little or no attention. Informed decision making by health service clients is generally most widely promoted in Western industrialised countries. Often particular areas of health service provision are investigated (such as breast and prostate cancer treatments) and patients views are surveyed on the processes (Jeames & Huckaby 2007; Hawley 2007). These industrialised environments are often very different from those in developing countries: the higher standard of facilities and wider range of options available are provided in the contexts of better staff to patient ratios, better working conditions, and relative affluence. In developing countries facilitating informed decision making is more likely to apply to helping medical staff make decisions about good practice and patient care, for example by introducing new technology to increase access to up to date research (Smith 2009). Health workers themselves, in both developing and developed countries, seem rarely consulted about the challenging environments they work in. The research commissioned by Cordaid to investigated how health providers in faith-based agencies manage to support their clients in sexual health decision making will provide valuable insights into the perspective of service providers; and the overlapping religious, cultural, legal, and contextual influencing factors on them as they strive to deliver HIV prevention, sexual health and family planning services. The research will identify the extent to which condoms are discussed as part of family planning options. Condom use in most Asian countries is very low among non-married partners, and even lower among married couples, and unpopular as a contraceptive option. In some cases (e.g. Thailand, Laos PDR and Indonesia) the aggressive promotion of condoms among sex workers has created a situation where condoms are synonymous with paid sex. It has become is a sign of grave mistrust to suggest condom use within a relationship (Kaybryn 2009). This may be the case in some parts of Africa too, but access to condoms appears to be hindered mostly by their lack of availability, their cost, as well as traditional values about fertility (WHO/USAID 2008). The research will ascertain whether condoms play a significant role in family planning among the participating partners. It is difficult to compare regions and identify transferable lessons. For example, the high proportions of Catholic women in Latin America that access modern contraceptives are likely to do so for many reasons: not least because of their availability. Secondly how people perceive the role of the Church and its leaders will correlate with their influence in peoples daily lives particularly in South America where liberation theology has a history of advocating for the rights of people in poverty. Its role, therefore, is one of promoting human rights and justice at national policy level, rather than influencing the day to day lives of individuals. In North America and Europe the rights of the individual are culturally highly valued. Therefore people perceive it as their right to follow a religions rules to the letter or, make decisions contrary to doctrine and still remain part of the religion. Even where religion is closely linked to politics, such as in Ireland where abortions are illegal, many women choose to travel to the UK or another country where abortions are legal.
28
10 June 2009 Plurpol Consulting
What is clear is that the environments that health providers operate in, no matter which continent or country, are likely to contain a range of political, cultural and religious influencing factors. What this research seeks to understand is the impact of these factors for nine partner organisations in three African countries. The research will ascertain the level of faith and religion (doctrine) that interacts with the programmes, and how health staff manage the (sometimes competing) demands placed on them by various hierarchies within and outside the organisations. At the same time, partner programmes will also be engaged in discussion about informed decision making how they facilitate this in the context of sexual and reproductive health provision.
29
10 June 2009 Plurpol Consulting
Annex: Summary of the research methodology
The research will seek to address many of the issues raised in this literature review. Inevitably not all will be responded to in depth through the research. Examples are provided through this document where the research will address specific areas. The research takes place in two parts. A summary of the methodology is given below:
Part One: field research by in-country researchers
Firstly in-country researchers will spend approximately one week with each partner using a variety of methodologies to understand their practice.
Observation of the facility
A checklist is provided in order to understand the environment in which the staff work and its impact on the service that they are able to provide. It is also designed to understand the environment in which clients receive the service. The first set of indicators can be observed directly, such as the privacy of the counselling rooms, and the public health messages displayed in waiting rooms. The second set of indicators on working conditions may be observed and may also require making enquiries over the course of the visit, such as the numbers and gender ratio of staff, their average working hours and ranges of responsibilities.
Questionnaire for clients
The questionnaire serves two purposes: firstly to verify information about service providerclient interaction and secondly to collect data on the attitudes of clients to better understand the context that the staff provide their services in. Research assistants will invite clients to complete the survey after their visit.
Focus group discussion with clients
The discussion with a group of clients allows for the opportunity of finding out in more detail what the experience of clients at the service provider consists of; whether the clients hold religious views themselves; and whether they feel that the service provision is influenced (and should be influenced) by religious values.
Direct observation of client-service provider interaction
In order to record the kinds of information that staff provide, and how they facilitate informed decision making, consent will be sought with clients (and staff) for the researcher to sit in on sessions. The researcher will note on a check list the reason for the visit, which information was provided, whether clients were supported to make decisions etc. This part of the research methodology poses some particular challenges because firstly, consent from clients may be difficult to obtain; and secondly such overt observation may affect the behaviour of both the client and the service provider. However, despite these potential biases the methodology will give us a better insight into the interaction, then no observation at all.
Interviews with senior staff/ head of partner organisation
This is a semi structured interview which will be important to ascertain the views of the organisations leadership. The head of the organisation will hopefully have a wider view of the external influences on the service provision. At the same time the views of the leadership will also be compared with the views of the staff members who interact with the clients to see if there is disparity or similarity between them.
30
10 June 2009 Plurpol Consulting
Participatory workshop with staff
This will be an in-depth study of how staff understand the factors that allow informed decision making to take place. Session 1: Group discussion on enabling and challenging factors This session takes participants through the five key areas of informed decision making as defined by Engender Health: A. Service options are available B. The decision making process is voluntary C. Individuals have appropriate information D. Good client-provider interaction, including counselling, is ensured E. The social and rights context support autonomous decision making The participants will be asked to discuss each element in detail, and consider each on three levels: personal/community; service delivery; and policy. Discussion of the five areas will reveal what the views and practice of the service providers are, and the influencing factors, including religion but also legal, financial and social impacts. Session 2: Self assessment exercise The self assessment tool will allow the staff to assess their current strengths and identify their priorities for areas of action. It takes each of the five key areas (A-E) which are needed for facilitating informed decision making, and suggests different levels of practice, from being aware of issues to systematising practice. Staff will identify which level they are currently at, and where they would like to progress to by 18 months time. The format is based on the AIDS Competence analysis tool which allows responses to be compared across organisations in order to see where learning and skills exchange can potentially take place. Session 3: Review session of main issues The final session with staff will be an opportunity to elicit from participants what the key determinants are for facilitating informed decision making in their faith based context.
Part Two: national workshops
The second part of the research will be a one day workshop with the three partner organisations in each country to feedback to them the data gathered to date, elicit further information on their practices, and begin to develop strategies for sharing good practice, particularly in the context of sharing the self assessment tool results.
31
10 June 2009 Plurpol Consulting
Annex: Documentation reviewed in this survey
African Union Health Strategy (2007-2015) Ambasa, C.R. The Impact of Culture Religion and Policy on the Reproductive Health of Women in Kenya, Kenyatta University, Kenya, prepared for CODESRIAs 10th General Assembly on Africa in the New Millennium, Kampala, Uganda, 8-12 December 2002 Beekman, M & Beest, J.T. Psychosocial problems of children on ARV treatment, Utrecht University, June 2007 Belden Russonello & Stewart. Religion, Reproductive Health and Access to Services: A National Survey of Women, Conducted for Catholics for a Free Choice, April 2000 Biriwasha, M. An Uneasy Relationship: Sex and Religion, www.realitycheck.org, September 2008 Browder. UNAIDS Attack on Church Is Unscientific, National Catholic Register, 2007 Burket, M.K. Advancing Reproductive Health and Family Planning through Religious Leaders and Faith-Based Organizations, Pathfinder International, August 2006 CAFO. Church Alliance Strengthens Support of Orphans and Vulnerable Children in Namibia, 2004 C-FAM, 'Catholic' Aid Organization in Holland Supports Plan to Promote Abortion, Volume 8, Number 32, July 29, 2005
CFC, Catholic Attitudes on Condoms in the Prevention of HIV and AIDS: Analysis of a survey in five nations for Catholics for Choice, Catholics for Choice, Washington, DC, 2007
CFC. The Catholic Bishops and Condoms: Statements and Actions Opposing Condom Use as Part of an HIV Prevention Strategy, accessed 21 March 2009 CFC. The Catholic Bishops and Condoms: Statements and Actions Supporting Condom Use as Part of an HIV Prevention Strategy, accessed 21 March 2009 Christian Aid. (Mary Garvey), Dying to learn: Young people, HIV and the churches Christian Aid, 2003 Cordaid. Directors speech to DRC partners, no date Cordaid. Report of Zambia HIV/AIDS Workshop, 2007 Cordaid, KENYA / Marsabit and Moyale District programme summary: Enhancing community participation in health services provision, no date, accessed:
http://cordaid.so-creatief.nl/Projecten2007/middle.php?id=21&PHPSESSID=90b036a8bbb6a4a52b0ec2fafc6d0dc4
COS Noord-Holland, COS Zeeland, Oxfam Novib, CINI Holland, Appointments and Agreements on MDG 5 Are we doing well regarding Millennium Development Goal 5?, 15 October 2008 de la Torre, S. Adolescent Group Male Circumcision: The experience of faith based hospitals in Kenya, Global Health Council, May 2008 de Waal, M. Turning the Tide: A qualitative study of SACBC funded antiretroviral treatment programmes, University of Pretoria, January 2005 Dowling, K. Bishop Kevin Dowling, AIDS and the God of Healing, no date Drost, R & Wierda, T. 'Quality of Life' study experiences article, University of Utrecht & Southern African Bishops Conference (SACBC) AIDS Desk, September-November 2006
32
10 June 2009 Plurpol Consulting
EAA. The Next Steps: For positive change in attitudes that cause HIV and AIDS-related stigma and discrimination. Ecumenical Advocacy Alliance 2003 Ecumenical Pharmaceutical Network, Nairobi, Kenya 2006 Episcopal Conference of Malawi, Be a Leader: Stop AIDS; Keep the Promise, 2007 FHI, Family Life Education: Teaching Adults to Communicate with Youth from a Christian Perspective, Family Health International 2006a FHI, Family Life Education: Teaching Adults to Communicate with Youth from a Muslim Perspective, Family Health International 2006d FHI, Family Life Education: Teaching Youth about Reproductive Health and HIV/AIDS from a Christian Perspective, Family Health International 2006b FHI. (William L. Sachs), Empowered by Faith - Collaborating with Faith-Based Organizations to Confront HIV/AIDS, Family Health International 2007 FHI. Family Life Education: A Handbook for Adults Working with Youth from a Christian Perspective, Family Health International 2006c Fikelela AIDS Project (Revd Rachel March and Mrs Roselyn Kareithi), Youth and Sexuality Research Ages 12-19 years in the Diocese of Cape Town South Africa, July 2005 Foster, G. From the Ground Up: Building Comprehensive HIV/AIDS Care Programs in Resource-Limited Settings, Ed by Richard G. Marlink, and Sara J. Teitelman, Elizabeth Glaser Pediatric AIDS Foundation, 2008 Gerald Clarke, Faith Matters: Development and the Complex World of Faith-Based Organisations, Centre for Development Studies, University of Wales, Swansea, September 2005 Green, E.C. Faith-Based Organizations: Contributions to HIV Prevention, Harvard Center for Population and Development Studies & U.S. Agency for International Development, September 2003 Haddad B, Olivier J, De Gruchy S. The potential and perils of partnership: Christian religious entities and collaborative stakeholders responding to HIV and AIDS in Kenya, Malawi and the DRC. Study commissioned by Tearfund and UNAIDS. African Religious Health Assets Programme (ARHAP) 2008 Harth, E. The impact of religion on sexual and reproductive health and rights in Latin America, Catholics for Choice, circa 2008 Hawley S, Janz N, Hamilton A, Katz SJ. Latina patient perspectives about informed decision making for surgical breast cancer treatment, Journal of Clinical Oncology, 2007 ASCO Annual Meeting Proceedings Part I. Vol 25, No. 18S (June 20 Supplement), 2007: 6544 IDS (Henry Armas), Policy Briefing: Sexuality and Development, April 2006 IDS (Henry Armas), Whose Sexuality Counts? Poverty, Participation and Sexual Rights, November 2007 IDS, Rethinking sexuality and policy, id21 insights issue 75, November 2008 Insideout Research, Siyamkela: Tackling HIV/AIDS stigma: Guidelines for faith-based organisations, Joint publication by POLICY Project, South Africa, Centre for the Study of AIDS, University of Pretoria; United States Agency for International Development (USAID); and Chief Directorate: HIV, AIDS & TB, Department of Health, 2003 INTRAC, HIV in the workplace: 20 ways for INGOs to help partners, 2009 IPPF & ASFP, Religion and commodities fact sheet, 2008b
33
10 June 2009 Plurpol Consulting
IPPF & ASFP, Religion and reproductive health fact sheet, 2008a Jeames & Huckaby, Prostate Cancer: informed decision making and cancer resources, National Institutes of Health, 2007 Kaybryn, J. Rapid Assessment of Feminisation of AIDS and Spousal Transmission of HIV in Indonesia, Laos and Thailand, UNICEF, forthcoming 2009. Kelly, M.J. Addressing the Susceptibility of Youth to HIV Infection, 2002 Keough, L & Marshall, K. Faith Communities Engage the HIV/AIDS Crisis - Lessons Learned and Paths Forward, Berkley Center for Religion, Peace and World Affairs, Georgetown University, 2007 Lambrechts, D. Working together ecumenically around AIDS, Southern African Catholic Bishops Conference (SACBC) AIDS Office, May 2007 Munro, A. Belated but Powerful, Southern African Catholic Bishops Conference (SACBC) AIDS Office, 2002 Munro, A. Catholic Social Teaching and our Response to AIDS, Southern African Catholic Bishops Conference (SACBC) AIDS Office, Pretoria, October 2008 Munro, A. Church, State, Society? Whose Responsibility is AIDS?, Southern African Catholic Bishops Conference (SACBC) AIDS Office, October 2003 Munro, A. In conversation with the Catholic Church: a response to AIDS Southern African Catholic Bishops Conference (SACBC) AIDS Office, 2005b Munro, A. Sisters for Sisters Religious Congregations affected and infected by AIDS, Southern African Catholic Bishops Conference (SACBC) AIDS Office, 2004 Munro, A. The Catholic Church and the provision of antiretroviral treatment, Southern African Catholic Bishops Conference (SACBC) AIDS Office, 2005a National Childrens Bureau, Faith, values and sex and relationships education - Fact Sheet, 2004 National Childrens Bureau, Faith, values and sex and relationships education, Sex Education Forums Factsheet, 2002 NBR (Laura M. Kelley and Nicholas Eberstadt), Special Report - Behind the Veil of a Public Health Crisis: HIV/AIDS in the Muslim World, June 2005 NCR. National Catholic Reporter, Pope addresses corruption, conflict in Africa, John L Allen Jr, 17 March 2009 Nubuasah, F. Salvation and Liberation in Africa, Bishop of Francistown, October 2006 October 2008 Catholic Social Teaching and AIDS Oct 2008.pdf http://www.sacbc.org.za/Site/index.php?option=com_content&task=view&id=117&Itemid=136 Parry, S. Responses of the churches to HIV and AIDS in South Africa, World Council of Churches, 2005 Paterson, G. AIDS Related Stigma: Thinking Outside the Box, Ecumenical Advocacy Alliance & World Council of Churches, 2005 Pearson, PJ. HIV/AIDS and Catholic Social Thought, Southern African Catholic Bishops Conference (SACBC) AIDS Office, May 2007 Phalana, V. Our pastoral response to the HIVAIDS pandemic, Southern African Catholic Bishops Conference (SACBC) AIDS Office, 2007
34
10 June 2009 Plurpol Consulting
PLANetWIRE, The Religious Consultation on Population: Religion and Reproductive Health and Rights, Media Summary, April 2005 Population Council (Ravai Marindo, Steve Pearson, John B. Casterline), Condom Use and Abstinence Among Unmarried Young People in Zimbabwe: Which Strategy, Whose Agenda? 2003 Positive Muslims (Farid Esack, Shahrukh Alam and Kabir (Sanjay) Bavikatte) , HIV, AIDS and Islam: A Workshop Manual Based on Compassion, Responsibility and Justice, 2007 Positive Muslims, HIV, AIDS & Islam, Reflections based on Compassion, Responsibility & Justice, 2004 Regnerus, M. and Trinitapoli, J. Village Sexual Norms and Links between Religion and HIV Infection Risk in Rural Malawi, Department of Sociology and Population Research Center, University of Texas at Austin, presented at the Population Association of America Annual Meeting, 2006 Runeborg, A. Sexuality: A Missing Dimension in Development, SIDA, May 2008 Ryan, C.P. AIDS, Ethics and Conscience, Southern African Catholic Bishops Conference (SACBC) AIDS Office, 2007 Say, L & Raine, R. A systematic review of inequalities in the use of maternal health care in developing countries: examining the scale of the problem and the importance of context, WHO Bulletin Volume 85, Volume 10, October 2007, 733-820 SECAM, A proposed HIV/AIDS Plan of Action by SECAM meeting of secretaries general held in Johannesburg, South Africa, 24th 27th October 2002 Smith, A, Maher, J, Simmons, J, Dolan, M. HIV Prevention from the Perspective of a Faith-Based Development Agency, CAFOD 2004 Smith H. Access to Electronic Health Knowledge in Africa, Liverpool School of Tropical Medicine, 2009 Speicher, S and Wilson, J. Exploring Solutions: How to Talk about HIV Prevention in the Church, Ecumenical Advocacy Alliance, 2007 Stonewall (Ruth Hunt & G Valentine), Love Thy Neighbour: What people of faith really think about homosexuality, 2008 Tanner, NP. Ed. Decrees of the Ecumenical Councils. 2 volumes. Washington, DC: Georgetown University Press, 1990 Taylor, N. DFID, faith and AIDS: A Review for the Update of Taking Action. A desk review prepared for The UK Consortium of AIDS & International Development Faith Working Group - Thembisa Development Consulting, 2007 Tearfund, Working Together? Challenges and opportunities for international development agencies and the church in the response to AIDS in Africa, HIV and AIDS briefing paper 7, August 2006 Thoraya Ahmed Obaid, Population and Reproductive Health: Culture and religion matter, 8th General Assembly Asian Forum of Parliamentarians on Population and Development, Statement by Executive Director UNFPA, 12 November 2005 Trinitapoli, J & Regenerus, M.D. Religion and HIV Risk Behaviors Among Married Men: Initial Results from a Study in Rural Sub-Saharan Africa, 2006 Trinitapoli, J. Religion and HIV Status in Sub-Saharan Africa: Examining Influence and Pathways, University of Texas at Austin, presented at the Population Association of America Annual Meeting, 2006
35
10 June 2009 Plurpol Consulting
UNAIDS, AIDS education through Imams - A spiritually motivated community effort in Uganda, UNAIDS Case Study, October 1998 UNFPA, Culture and religion, HIV/AIDS Update 2002 UNFPA, Culture in the Context of UNFPA Programming: ICPD+10 Survey Results on Culture and Religion, United Nations Population Fund, 2005 UNFPA, Culture Matters: Working with Communities and Faith-based Organizations: Case Studies from Country Programmes, United Nations Population Fund, 2004 UNICEF, Study of the Response by Faith-Based Organizations to Orphans and Vulnerable Children, Compiled by Geoff Foster, World Conference of Religions for Peace & United Nations Children Fund, 1995 UNICEF, What religious leaders can do about HIV/AIDS: Action for Children and Young People - United Nations Childrens Fund 2003 USAID, Mobilizing Muslim Religious Leaders for Reproductive Health and Family Planning at the Community Level: A Training Manual, circa 2007 van Beuningan, C. Ashtrays in Sports Cars: Parameters for a catholic policy agenda in HIV-AIDS care, Cordaid, 2006 Vatican, Considerations regarding proposals to give legal recognition to unions between homosexual persons, 2003 Vatican, Family, marriage and de facto unions, 2000 Vatican, Humanae Vitae, 1968 WHO/USAID, Repositioning Family Planning: Guidelines for advocacy action, 2008 WHO/UNAIDS, New Data on Male Circumcision and HIV Prevention: Policy and Programme Implications, March 2007 WHO, Multi-Country Study of Medicine Supply and Distribution Activities of Faith-Based Organizations in SubSaharan African Countries, Department of Medicines Policy and Standards, World Health Organization 2006 Wolfensohn, J.D. Millennium Challenges for Faith and Development: New Partnerships to Reduce Poverty and Strengthen Conservation, World Bank Group, 30 March 2004 Wood, R. Implementation of ARV therapy in faith-based clinics, Southern African Catholic Bishops Conference (SACBC) AIDS Office, August 2007 World Association for Sexual Health, Sexual Health for the Millennium: A Declaration and Technical Document, 2008 WWHR, Sexuality and human rights in Muslim societies, http://www.wwhr.org/sexuality_in_muslim_soc.php accessed 21 March 2009
36
10 June 2009 Plurpol Consulting
Annex: Recent statements on condoms by Catholic religious leaders
Source: Condoms4Life, "The Catholic Bishops and Condoms: Statements and Actions Supporting Condom Use to Prevent the Spread of HIV," Washington DC: Catholics for a Free Choice, 2006
The Catholic Bishops and Condoms: Statements and Actions Supporting Condom Use as Part of an HIV Prevention Strategy Date March 2009 Bishop Bishop Hans-Jochen Jaschke, Hamburg, Germany Statements supporting condom use as part of HIV prevention Pope Benedicts deplorable comments, on a flight to Cameroon, opposing condom use to stop the spread of HIV/AIDS rightfully sparked a lot of opposition, including some from within the church hierarchy itself. Hans-Jochen Jaschke, a Catholic auxiliary bishop of Hamburg, Germany, spoke of the need for no taboo on the condom issue. He wisely declared that "anyone who has AIDS and is sexually active, anyone who seeks multiple partners, must protect others and themselves." Cardinal Peter Turkson of the Cape Coast in Ghana has advocated that priests take on more of a counseling role in discussing condom use with married couples in which one of the partners is HIV positive. Acknowledging the hierarchys teachings on conscience, he suggested help[ing] the client to take the decision which [he or she] will be at peace with. According to Turkson, the issue is being seriously debated by bishops conferences in Africa, but he has been slow to publicly support condom use from the pulpit, indicating that he will only speak in person-to-person counseling, allowing those who can, to choose for love of their partner to abstain, and those who also for love of their partner may want to use this way [condoms]. Bishop Dowling, in an interview about HIV/AIDS prevention and treatment in South Africa said, "Abstinence before marriage and faithfulness in a marriage is beyond the realm of possibility here. The issue is to protect life. That must be our fundamental goal." Drawing attention to the especially difficult plight of women in the traditionally male-dominated societies of his diocese he continued, "My passion is for the women. I'm in that corner." About the African people, he says, "They must use condoms," maintaining his stance despite the Vaticans continued opposition to such a policy. Following the release of a report showing that among all religious people, Catholics are the most supportive of the use of condoms for contraception and preventing sexually transmitted diseases, Mombassa Archbishop Boniface Lele said, With some counselingand this is something we dont tell everyoneyou can ask couples to use condoms, so that the rate of reinfection goes down. Source Philip Pullella, "Vatican Defends Pope Condoms Stand, Criticism Mounts." Reuters, March 18, 2009.
October 2007
Cardinal Peter Turkson, Cape Coast, Ghana
James Roberts, African church leader advocates pastoral approach on condom use. The Tablet, October 20, 2007.
April 2007
Bishop Kevin Dowling, South Africa
Bishop promotes condoms use; In South Africa town, issue is protecting life, not preventing pregnancy, Grand Rapid Press (Michigan), April 15, 2007.
August 2006
Archbishop Boniface Lele, Kenya
Topi Lyambila & Agencies, Kenyan Catholics Support Condoms More Than Other Faith Groups, Kenya London News, August 25, 2006.
37
10 June 2009 Plurpol Consulting
Date May 2006
Bishop Cardinal Christian Wiyghan Tumi, Cameroon
Statements supporting condom use as part of HIV prevention In an interview with Deutsche Presse-Agentur, the archbishop of Douala, Cardinal Christian Wiyghan Tumi, defended the decision to use condoms to prevent the transmission of HIV/AIDS between married couples, saying, If a partner in a marriage is infected with HIV, the use of condoms makes sense. In an interview with a Scottish newspaper, Mario Conti, the Archbishop of Glasgow, pledges his support for the Pontifical Council for Health Care Workers' recent decision to conduct and release a study on condom use to fight AIDS and contends that using condoms to stop transmission of the disease from one spouse to another is "common sense." He acknowledges that this position is not in line with church teaching, but asks, "Should we really be saying that it is in the benefit of the couple to refuse one anotherand [live] as brother and sister when the whole nature of their marriage pushes them towards sacramentalising their marriage?" South African Bishop Kevin Dowling addresses a forum sponsored by Physicians for Human Rights about the use of condoms in preventing the spread of AIDS. While he reiterates the important place that fidelity and abstinence before marriage can have in stopping the deadly virus, he maintains that this approach alone is not a pragmatic solution based in the realities of people's lives around the world. He insists, "Abstinence is fine as an ideal, but it does not work in all circumstances.... We have to try a more holistic approach, a theology and possibility for people to encounter God right within their situation." Speaking at a meeting of Portuguese bishops held in the town of Fatima, about 85 miles from Lisbon, Bishop Antonio Moreira, vice president of the Portuguese episcopal conference, says, "In a context of marriage where one or both are infected, the use of a condom is a clear case of a lesser evil." In an interview with the Italian magazine L'espresso, Cardinal Carlo Maria Martini, the retired Archbishop of Milan, says, "Certainly the use of prophylactics can, in some situations, constitute a lesser evil. There is the particular situation of spouses, one of whom is affected by AIDS. It is the obligation of this spouse to protect the other partner and they must be able to protect themselves." In recognition of a growing AIDS problem in Papua New Guinea, Bishop Gilles Cote, the head of the Daru-Kiunga Diocese in Western Province, conceded that it may be wise for the government to provide condoms. Speaking to the Vaticans ban on contraception, he argued, We also have a law you should not killso there is a moral responsibility that [those with a partner who is infected] are
Source Cardinal Endorses Condoms for Married Couples, The Tablet, May 11, 2006.
May 2006
Archbishop Mario Conti, Scotland
Stephen McGinty, "Archbishop believes condoms are 'commonsense' in the war on AIDS," The Scotsman, May 5, 2006.
April 2006
Bishop Kevin Dowling, South Africa
Nora Boustany, "AIDS Crisis Shapes Bishop's Stance," Washington Post, April 26, 2006.
April 2006
Bishop Antonio Moreira, Portugal
Agence France-Presse, "Portuguese Catholic bishop backs call to ease ban on condoms," April 28, 2006. Peter Popham, "Pope John Paul II Seen by Many as Main Obstacle for Change," Independent (UK), May 3, 2006. Lloyd Jones, PNG: Facing AIDS epidemic, bishop says condoms okay for some, AAP Newsfeed, March 29, 2006.
April 2006
Cardinal Carlo Maria Martini, Italy
March 2006
Bishop Gilles Cote, Papua New Guinea
38
10 June 2009 Plurpol Consulting
Date
Bishop protected.
Statements supporting condom use as part of HIV prevention
Source
The Catholic Bishops and Condoms: Statements and Actions Opposing Condom Use as Part of an HIV Prevention Strategy Date February 2009 Bishop Cardinal Cormac Murphy O'Connor Statements opposing condom use as part of HIV prevention Cardinal Cormac Murphy OConnor, the Archbishop of Westminster, heartlessly asserted that it is quite ridiculous to go on about Aids in Africa and condoms. According to OConnor, there are much more important things, including education, healthcare, and abstinence. He also furthered the myth that condoms can cause HIV/AIDS, stating that his diocese is flooded with condoms and there is more AIDS because of them. Bishop Demetrio Fernandez of Tarazona, Spain, has absurdly claimed that the Catholic Church is leading the fight against HIV/AIDS by denouncing condom use and encouraging abstinence. According to Fernandez, The condom is a cork, and is not always effective. He went so far as to say that in the field of AIDS, as in all fields that include the proper use of sexuality, the Church presents the proposal of true love, which brings with it a proper education in the virtue of chastity. Bishop Hugh Slattery of Tzaneen, South Africa, recently expressed a multi-step plan for reducing the high rate of HIV/AIDS in his country that unrealistically focuses on abstinence only. He stated that the first step is to make everyone aware of the problem and the next involves showing that abstinence before marriage and fidelity within marriage will quickly stop the spread of AIDS. Despite his narrow approach, he even suggested, As a Church, we are trying to lift the veil of secrecy and denial around HIV/AIDS and get people to talk about it openly. The archbishop of Chimoio has accused European condom makers of intentionally trying to spread AIDS in Africa. According to Chimoio, the condoms being sent to Africa are first contaminated with HIV in order to finish quickly the African people. It is estimated that one in six people in Mozambique is HIV positive. While the comments have earned attention, ridicule and reprove worldwide, the Vatican has been silent on the subject, failing to publicly reprimand the archbishop or even denounce his accusations. During the first national Catholic conference on HIV/AIDS in Nairobi, Bishop Sulumeti stated that the Source Times (London), "Cardinal Cormac Murphy O'Connor: Recession May be Jolt that Selfish Britain Needs," February 14, 2009.
August 2008
Bishop Demetrio Fernandez of Tarazona, Spain
Catholic News Agency, "Church Proposes More Effective Approach to AIDS, Spanish Bishop Says," August 11, 2008.
January 2008
Bishop Hugh Slattery of Tzaneen, South Africa
Zenit, "Common Sense in Fighting AIDS," January 9, 2008.
September 2007
Archbishop Francisco Chimoio, Maputo, Mozambique
BBC News, "Shock at archbishop condom claim." September 26, 2007.
June 2007
Bishop Philip Sulumeti of
Catholic Information Service for
39
10 June 2009 Plurpol Consulting
Date
Bishop Kakamega Diocese, chairman of the Kenya Episcopal Conference's Commission for Health
Statements opposing condom use as part of HIV prevention Catholic Church opposed all forms of contraceptives. In reference to the difficult situation faced by couples where in one partner is HIV positive, he stated flatly, "Even in the case of discordant couples [where one spouse is infected], those offering care should look at all the issues affecting the couple other than the sexual aspect. One of them will have to sacrifice for the sake of the other." Cardinal Egan chided the New York City Department of Health and Mental Hygiene for its plan to distribute 18 million condoms to the public for free in an effort to curb the spread of HIV/AIDS and other sexually transmitted diseases. According to Egan, the citys initiative and encourages inappropriate sexual activity. In the months preceding the papal visit to Brazil, officials came under harsh attack from the countrys Roman Catholic hierarchy for the governments support of comprehensive sex education and a successful AIDS prevention program which distributes free condoms. On the television program Fantastico, Cardinal Majella, the head of the National Bishops Conference commented, We cannot agree with condoms because they turn life into a life without responsibility. In a later interview he added that the use of the condom encourages people to have inconsequential and irresponsible sex. In response to a comment made by Tony Blair on December 1, World AIDS Day, calling on the church to reassess its position on condom use, Cardinal Murphy OConnor criticized the prime ministers willingness to give more and more aid, including more condoms to Africa for AIDS prevention. According to the cardinal, African bishops he has spoken with claim their dioceses are flooded with condoms and it has meant more promiscuity and more AIDS. During the opening of the national religious leaders conference on stigma, denial and discrimination in Kenya, Archbishop Ndingi Mwana aNzeki urged the government to ban advertising and distributing condoms. He insisted, There are no two ways about it. When condoms are provided anyhowly, chances of promiscuity increase since a majority of our people end up engaging in casual sex. In an interview with the Sunday Times (Perth, Australia), Perth archbishop Barry Hickey condemned those who promote condoms as a means for safe sex saying, Society only gives false assurances to young peoplebecause the failure rate of condoms will eventually catch up with them and the consequences of intercourse will be there. Pregnancy is an obvious example but even as preventers
Source Africa, Kenya: Catholics Reaffirm Stand Against Condoms in Fighting HIV/AIDS," Africa News, June 26, 2007. National Catholic Reporter, Condom Giveaway, March 2, 2007.
March 2007
Cardinal Edward M Egan, New York
March 2007
Cardinal Geraldo Majella Angelo, Brazil
Reuters, Condom debate flares in Brazil before pope visit, March 12, 2007. Pravda, Brazilian government and church argue over condoms, March 13, 2007.
December 2006
Cardinal Cormac Murphy OConnor, Westminster
Ben Padley, Drugs Better than Condoms in AIDS Fight, Says Cardinal, Press Association, December 3, 2006.
November 2006
Archbishop Ndingi Mwana aNzeki, Nairobi
The Nation (Nairobi, Kenya), Stop Giving Free Condoms, Say Clerics, November 29, 2006.
November 2006
Archbishop Barry Hickey, Perth
Paul Lampathakis, Calls for Modest Dress, Less Sex, Sunday Times (Perth, Australia), November 13, 2006.
40
10 June 2009 Plurpol Consulting
Date
Bishop
Statements opposing condom use as part of HIV prevention of disease, condoms eventually fail. There is another answer and thats self-control and chastity.
Source
May 2006
Cardinal Alfonso Lopz Trujillo
In an interview for a Spanish newspaper, Cardinal Alfonso Lopz Trujillo discredits a statement made by Cardinal Carlo Maria Martini that the use of condoms for AIDS prevention is "a lesser evil," insisting that the statement was not reflective of the church's position. Despite confirmation given late in April by the President of the Pontifical Council for Health Pastoral Care, Cardinal Javier Lozano Barragn, Cardinal Trujillo also denied that Pope Benedict XVI ordered a study on condoms.
Nstor Pongut Puerto, "Por ahora no hay nada sobre la aceptacin del uso del preservative, El Pas, May 4, 2006, and John L. Allen, Jr., Vatican in Condom Debate, National Catholic Reporter, April 28, 2006. Africa News, "Catholic bishops reject school syllabus over condoms," January 13, 2006.
January 2006
Tanzanian Episcopal Conference
Tanzania's Episcopal Conference calls material on the Ministry of Education's recently released school science syllabus "sinful" because it includes the proper use of condoms as one way to prevent the spread of HIV/AIDS. In a statement issued on behalf of the conference, Cardinal Polycarp Pengo, the archbishop of Dar es Salaam, says the "introduction of the [teaching of] use of condoms in schoolsis indeed justification and opening the door for immoral lifestyles."
41
Anda mungkin juga menyukai
- UNICEF Assessing Child-Sensitivity in Social Protection: A Toolkit For Social TransfersDokumen204 halamanUNICEF Assessing Child-Sensitivity in Social Protection: A Toolkit For Social TransfersJo KaybrynBelum ada peringkat
- Evaluation of UNFPA's 8th Country Programme of Cooperation in Viet NamDokumen141 halamanEvaluation of UNFPA's 8th Country Programme of Cooperation in Viet NamJo KaybrynBelum ada peringkat
- Formative Evaluation UNICEF's Child Protection System Building Approach in IndonesiaDokumen152 halamanFormative Evaluation UNICEF's Child Protection System Building Approach in IndonesiaJo KaybrynBelum ada peringkat
- HIV Resources For Faith LeadersDokumen35 halamanHIV Resources For Faith LeadersJo KaybrynBelum ada peringkat
- Intimate Partner Transmission of HIV: IndonesiaDokumen2 halamanIntimate Partner Transmission of HIV: IndonesiaJo KaybrynBelum ada peringkat
- Qualitative Findings From Cambodia's Violence Against Children Survey 2013 (English)Dokumen64 halamanQualitative Findings From Cambodia's Violence Against Children Survey 2013 (English)Jo KaybrynBelum ada peringkat
- Quantitative Findings From Cambodia's Violence Against Children Survey 2013 (English)Dokumen210 halamanQuantitative Findings From Cambodia's Violence Against Children Survey 2013 (English)Jo Kaybryn100% (1)
- HIV-Sensitive Community Based Health InsuranceDokumen12 halamanHIV-Sensitive Community Based Health InsuranceJo KaybrynBelum ada peringkat
- HIV Sensitive Social Protection: A Review of Cambodia's Social Protection Schemes For Incorporating HIV Sensitivity (English)Dokumen64 halamanHIV Sensitive Social Protection: A Review of Cambodia's Social Protection Schemes For Incorporating HIV Sensitivity (English)Jo KaybrynBelum ada peringkat
- Buddhist Leadership Initiative Evaluation 2008-2012, Cambodia (English)Dokumen84 halamanBuddhist Leadership Initiative Evaluation 2008-2012, Cambodia (English)Jo KaybrynBelum ada peringkat
- Intimate Partner Transmission of HIV: ThailandDokumen2 halamanIntimate Partner Transmission of HIV: ThailandJo KaybrynBelum ada peringkat
- A Mapping of Faith-Based Responses To Violence Against Women and Girls in The Asia Pacific RegionDokumen80 halamanA Mapping of Faith-Based Responses To Violence Against Women and Girls in The Asia Pacific RegionJo KaybrynBelum ada peringkat
- Zambia: What People Living With and Affected by HIV Want From Their Faith Leaders: Reflections and Data On Stigma Experienced by Faith CommunitiesDokumen1 halamanZambia: What People Living With and Affected by HIV Want From Their Faith Leaders: Reflections and Data On Stigma Experienced by Faith CommunitiesJo KaybrynBelum ada peringkat
- Intimate Partner Transmission of HIV: Lao PDRDokumen2 halamanIntimate Partner Transmission of HIV: Lao PDRJo KaybrynBelum ada peringkat
- HIV and Maternal Health: Annex 2Dokumen6 halamanHIV and Maternal Health: Annex 2Jo KaybrynBelum ada peringkat
- Addressing The Silent Emergency: HIV and AIDS and The Darfur CrisisDokumen2 halamanAddressing The Silent Emergency: HIV and AIDS and The Darfur CrisisJo KaybrynBelum ada peringkat
- HIV and Maternal Health: Annex 1Dokumen68 halamanHIV and Maternal Health: Annex 1Jo KaybrynBelum ada peringkat
- HIV and Maternal Health: Faith Groups' Activities, Contributions and ImpactDokumen94 halamanHIV and Maternal Health: Faith Groups' Activities, Contributions and ImpactJo KaybrynBelum ada peringkat
- Sinethemba: We Have Hope. A Reflection by CAFOD Partners in South Africa On Responding To Children Affected by HIV and AIDSDokumen52 halamanSinethemba: We Have Hope. A Reflection by CAFOD Partners in South Africa On Responding To Children Affected by HIV and AIDSJo KaybrynBelum ada peringkat
- What People Living With and Affected by HIV Want From Their Faith Leaders Reflections and Data On Stigma Experienced by Faith Communities in Ethiopia, Kenya, and ZambiaDokumen1 halamanWhat People Living With and Affected by HIV Want From Their Faith Leaders Reflections and Data On Stigma Experienced by Faith Communities in Ethiopia, Kenya, and ZambiaJo KaybrynBelum ada peringkat
- Ethiopia: What People Living With and Affected by HIV Want From Their Faith Leaders: Reflections and Data On Stigma Experienced by Faith CommunitiesDokumen1 halamanEthiopia: What People Living With and Affected by HIV Want From Their Faith Leaders: Reflections and Data On Stigma Experienced by Faith CommunitiesJo KaybrynBelum ada peringkat
- Emergency Response Kit: Manual of ProcedureDokumen60 halamanEmergency Response Kit: Manual of ProcedureJo KaybrynBelum ada peringkat
- Informed Decision Making: A Guide For Partner Organisations Providing Sexual and Reproductive Health ServicesDokumen2 halamanInformed Decision Making: A Guide For Partner Organisations Providing Sexual and Reproductive Health ServicesJo KaybrynBelum ada peringkat
- Intergenerational Poverty and Social ProtectionDokumen15 halamanIntergenerational Poverty and Social ProtectionJo KaybrynBelum ada peringkat
- Evaluation of The Impact of Christian Aid's Support of Faith Based Responses To HIVDokumen30 halamanEvaluation of The Impact of Christian Aid's Support of Faith Based Responses To HIVJo KaybrynBelum ada peringkat
- HIV and AIDS and Older People in Developing CountriesDokumen13 halamanHIV and AIDS and Older People in Developing CountriesJo KaybrynBelum ada peringkat
- The National HIV Response of Indonesia: Gender and Human Rights ReviewDokumen57 halamanThe National HIV Response of Indonesia: Gender and Human Rights ReviewJo KaybrynBelum ada peringkat
- Gender Power Dynamics in Marriage and HIV Sero-Discordant RelationshipsDokumen54 halamanGender Power Dynamics in Marriage and HIV Sero-Discordant RelationshipsJo KaybrynBelum ada peringkat
- Presentation: National Review of Faith-Based Responses To HIV in Cambodia (English)Dokumen16 halamanPresentation: National Review of Faith-Based Responses To HIV in Cambodia (English)Jo KaybrynBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- "An Order Establishing The Implementing Team Fo The ResponsibleDokumen5 halaman"An Order Establishing The Implementing Team Fo The ResponsibleBarangay CatoBelum ada peringkat
- No Woman Should Die Giving LifeDokumen112 halamanNo Woman Should Die Giving LifelibremdBelum ada peringkat
- Breaking The VowsDokumen40 halamanBreaking The VowsPlan Sverige100% (1)
- Concept Framework Male Involvement in FPDokumen1 halamanConcept Framework Male Involvement in FPRadomir18Belum ada peringkat
- Unit II Lesson I: On Responsible Parenthood and PornographyDokumen22 halamanUnit II Lesson I: On Responsible Parenthood and PornographyKizea JuanicoBelum ada peringkat
- Local Youth Development Plan 2.0Dokumen3 halamanLocal Youth Development Plan 2.0Emmanuel Mascuñana Bacay100% (1)
- Joyce CV 2017Dokumen5 halamanJoyce CV 2017kevin muchungaBelum ada peringkat
- Chap. 2 LESSON 1-2 HealthDokumen16 halamanChap. 2 LESSON 1-2 HealthKalabit PengeBelum ada peringkat
- Supreme Court Upholds Conscience Clause in Philippines RH LawDokumen25 halamanSupreme Court Upholds Conscience Clause in Philippines RH Lawsheridan DienteBelum ada peringkat
- Eliminating Teenage Pregnancy in The Philippines: Policy BriefDokumen6 halamanEliminating Teenage Pregnancy in The Philippines: Policy BriefMari LeianaBelum ada peringkat
- Ped4141 Curriculum Map Final Copy - Cole Blanchard 1Dokumen24 halamanPed4141 Curriculum Map Final Copy - Cole Blanchard 1api-504523580Belum ada peringkat
- Sexual and Reproductive Health and Rights of Women in Nepal (SRHR)Dokumen12 halamanSexual and Reproductive Health and Rights of Women in Nepal (SRHR)Women’s Rehabilitation Centre (WOREC Nepal)Belum ada peringkat
- Research UkimDokumen10 halamanResearch UkimCyrus UrsuaBelum ada peringkat
- UNFPA-Adolescent Girls in Disaster Conflict-WebDokumen92 halamanUNFPA-Adolescent Girls in Disaster Conflict-WebsofiabloemBelum ada peringkat
- Health 9 Support PackageDokumen21 halamanHealth 9 Support PackageAllyson SaxBelum ada peringkat
- San Jose Youth Development Plan 1.0Dokumen16 halamanSan Jose Youth Development Plan 1.0Emmanuel Mascuñana Bacay100% (1)
- Coordination Letter Signed 1Dokumen3 halamanCoordination Letter Signed 1HeizmaebrizBelum ada peringkat
- Bellizzi Et Al. (2019) - Adolescent Women With Unintended Pregnancy in Low - and Middle-Income CountriesDokumen21 halamanBellizzi Et Al. (2019) - Adolescent Women With Unintended Pregnancy in Low - and Middle-Income CountriesRadomir18Belum ada peringkat
- Peace Corps Life Skills and Leadership Manual M0098 (No Date) pp.400Dokumen400 halamanPeace Corps Life Skills and Leadership Manual M0098 (No Date) pp.400Accessible Journal Media: Peace Corps Documents100% (1)
- Social Determinants of Unintended Pregnancy and Maternal CareDokumen29 halamanSocial Determinants of Unintended Pregnancy and Maternal Carelestari pamungkas100% (1)
- Kenya Gender Training ManualDokumen94 halamanKenya Gender Training Manualadakit100% (1)
- A Comparison of EDSA I and EDSA IIDokumen4 halamanA Comparison of EDSA I and EDSA IIReymark B. Ibuña100% (2)
- NNHS - 2018 - Final Report PDFDokumen161 halamanNNHS - 2018 - Final Report PDFMohammed BoseBelum ada peringkat
- R.A. 10354Dokumen36 halamanR.A. 10354Donzzkie DonBelum ada peringkat
- SRHR An Essential Element of UHC SupplementAndUniversalAccess 27-Online PDFDokumen48 halamanSRHR An Essential Element of UHC SupplementAndUniversalAccess 27-Online PDFEmmanuelBelum ada peringkat
- Population Dynamics and Contraception-1Dokumen36 halamanPopulation Dynamics and Contraception-1Anivasa KabirBelum ada peringkat
- Maternal and Child Health NursingDokumen17 halamanMaternal and Child Health NursingSarah Jane MaganteBelum ada peringkat
- Family Planning TVC 2014Dokumen22 halamanFamily Planning TVC 2014Janette Anne Reyes MacaraigBelum ada peringkat
- National Health AgenciesDokumen40 halamanNational Health AgenciesMadhavi Moda100% (1)
- Quarter 3 Mapeh: Lesson 1 (Health)Dokumen7 halamanQuarter 3 Mapeh: Lesson 1 (Health)Jannie SantillanBelum ada peringkat