Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- MNT-Notes Pt. 2Dokumen58 halamanMNT-Notes Pt. 2leemon.mary.alipao8695Belum ada peringkat
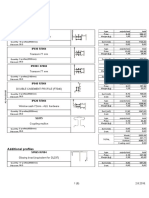
- Lista Materijala WordDokumen8 halamanLista Materijala WordAdis MacanovicBelum ada peringkat
- Experiment No 5 ZenerDokumen3 halamanExperiment No 5 ZenerEugene Christina EuniceBelum ada peringkat
- Demo StatDokumen5 halamanDemo StatCalventas Tualla Khaye JhayeBelum ada peringkat
- Instructional MediaDokumen7 halamanInstructional MediaSakina MawardahBelum ada peringkat
- BTS WORLD-Crafting GuideDokumen4 halamanBTS WORLD-Crafting GuideAn ARMYBelum ada peringkat
- Amy Kelaidis Resume Indigeous Education 2015 FinalDokumen3 halamanAmy Kelaidis Resume Indigeous Education 2015 Finalapi-292414807Belum ada peringkat
- Lsp404 How To Write An Argumentative Essay NewDokumen52 halamanLsp404 How To Write An Argumentative Essay Newagegae aegaegBelum ada peringkat
- ERP Test BankDokumen29 halamanERP Test BankAsma 12Belum ada peringkat
- Recurrent: or Reinfection Susceptible People: Adult With Low Im Munity (Especially HIV Patient) Pathologic ChangesDokumen36 halamanRecurrent: or Reinfection Susceptible People: Adult With Low Im Munity (Especially HIV Patient) Pathologic ChangesOsama SaidatBelum ada peringkat
- Jack Pumpkinhead of Oz - L. Frank BaumDokumen68 halamanJack Pumpkinhead of Oz - L. Frank BaumbobbyejayneBelum ada peringkat
- In Holland V Hodgson The ObjectDokumen5 halamanIn Holland V Hodgson The ObjectSuvigya TripathiBelum ada peringkat
- Sancticity AllDokumen21 halamanSancticity AllJames DeHart0% (1)
- Remo Vs DevanaderaDokumen2 halamanRemo Vs DevanaderaZymon Andrew MaquintoBelum ada peringkat
- 002 Constraints and Generalized Coordinates PDFDokumen27 halaman002 Constraints and Generalized Coordinates PDFNiveCeciliaBelum ada peringkat
- SANCHEZ V DEMETRIOUDokumen3 halamanSANCHEZ V DEMETRIOUShenna SunicoBelum ada peringkat
- Scanned - National Learning CampDokumen2 halamanScanned - National Learning CampJOHN JORICO JARABABelum ada peringkat
- Fundamentals of Biochemical Engineering Dutta Solution ManualDokumen6 halamanFundamentals of Biochemical Engineering Dutta Solution Manualhimanshu18% (22)
- Assignment in Legal CounselingDokumen4 halamanAssignment in Legal CounselingEmmagine E EyanaBelum ada peringkat
- Basic Foundation of Iv TherapyDokumen10 halamanBasic Foundation of Iv Therapyjanna mae patriarcaBelum ada peringkat
- Wardancer 4e HomebrewDokumen3 halamanWardancer 4e HomebrewWyjecBelum ada peringkat
- 145class 7 Integers CH 1Dokumen2 halaman145class 7 Integers CH 17A04Aditya MayankBelum ada peringkat
- Admission English Test 10thDokumen4 halamanAdmission English Test 10thEduardo100% (1)
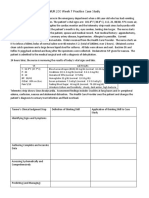
- NUR 200 Week 7 Practice Case StudyDokumen2 halamanNUR 200 Week 7 Practice Case StudyJB NicoleBelum ada peringkat
- Coaching Skills For Optimal PerformanceDokumen58 halamanCoaching Skills For Optimal PerformanceYodhia Antariksa100% (3)
- WE) The Accentual Structure of English WordsDokumen8 halamanWE) The Accentual Structure of English Wordszhannatagabergen2606Belum ada peringkat
- Types of Sutures and Their IndicationsDokumen6 halamanTypes of Sutures and Their IndicationsAdina BurciuBelum ada peringkat
- 89 Robinson V MirallesDokumen1 halaman89 Robinson V MirallesMartin AlfonsoBelum ada peringkat
- PRS Product DescriptionDokumen42 halamanPRS Product DescriptioneliaezekielBelum ada peringkat
- My AnalysisDokumen4 halamanMy AnalysisMaricris CastillanoBelum ada peringkat