Anda mungkin juga menyukai
- PFCD India Newsletter - August 2015Dokumen4 halamanPFCD India Newsletter - August 2015Partnership to Fight Chronic DiseaseBelum ada peringkat
- Diabetes Prevention Program - Fact SheetDokumen4 halamanDiabetes Prevention Program - Fact SheetPartnership to Fight Chronic DiseaseBelum ada peringkat
- Access To Medicines For Chronic Conditions On Access Health ConnecticutDokumen5 halamanAccess To Medicines For Chronic Conditions On Access Health ConnecticutPartnership to Fight Chronic DiseaseBelum ada peringkat
- The Science of Wellness Programs: A SynopsisDokumen53 halamanThe Science of Wellness Programs: A SynopsisPartnership to Fight Chronic Disease100% (1)
- Investing in Community HealthDokumen2 halamanInvesting in Community HealthPartnership to Fight Chronic DiseaseBelum ada peringkat
- Putting Patients FirstDokumen1 halamanPutting Patients FirstPartnership to Fight Chronic DiseaseBelum ada peringkat
- Improving Health and Wellness of Individuals: Spotlight On Verizon CommunicationsDokumen2 halamanImproving Health and Wellness of Individuals: Spotlight On Verizon CommunicationsPartnership to Fight Chronic DiseaseBelum ada peringkat
- Health and Wellness: Foundational Pillars and Priorities - VerizonDokumen1 halamanHealth and Wellness: Foundational Pillars and Priorities - VerizonPartnership to Fight Chronic DiseaseBelum ada peringkat
- UnhealthyTruths - CaliforniaDokumen19 halamanUnhealthyTruths - CaliforniaPartnership to Fight Chronic DiseaseBelum ada peringkat
- A Multi-Stakeholder Vision For Patient-Centered Measurement in New Payment and Delivery ModelsDokumen38 halamanA Multi-Stakeholder Vision For Patient-Centered Measurement in New Payment and Delivery ModelsPartnership to Fight Chronic DiseaseBelum ada peringkat
- A Multi-Stakeholder Vision For Patient-Centered Measurement in New Payment and Delivery ModelsDokumen7 halamanA Multi-Stakeholder Vision For Patient-Centered Measurement in New Payment and Delivery ModelsPartnership to Fight Chronic DiseaseBelum ada peringkat
- The Future of Performance MeasurementDokumen18 halamanThe Future of Performance MeasurementPartnership to Fight Chronic DiseaseBelum ada peringkat
- The Full Economic Impact of Chronic Health ConditionsDokumen8 halamanThe Full Economic Impact of Chronic Health ConditionsPartnership to Fight Chronic DiseaseBelum ada peringkat
- Facilitating Full Employment Opportunity For Employees With Cancer: A Call To ActionDokumen14 halamanFacilitating Full Employment Opportunity For Employees With Cancer: A Call To ActionPartnership to Fight Chronic DiseaseBelum ada peringkat
- Addressing Our Senior Obesity CrisisDokumen1 halamanAddressing Our Senior Obesity CrisisPartnership to Fight Chronic DiseaseBelum ada peringkat
- Patient Declaration On Chronic Disease Prevention and Management in TurkeyDokumen2 halamanPatient Declaration On Chronic Disease Prevention and Management in TurkeyPartnership to Fight Chronic DiseaseBelum ada peringkat
- Obesity Awareness News ConferenceDokumen1 halamanObesity Awareness News ConferencePartnership to Fight Chronic DiseaseBelum ada peringkat
- Private Sector Approaches To Workforce Health and Well-BeingDokumen6 halamanPrivate Sector Approaches To Workforce Health and Well-BeingPartnership to Fight Chronic DiseaseBelum ada peringkat
- Well-Being Improvement For Federal EmployeesDokumen8 halamanWell-Being Improvement For Federal EmployeesPartnership to Fight Chronic DiseaseBelum ada peringkat
- Fighting Chronic Disease and ObesityDokumen2 halamanFighting Chronic Disease and ObesityPartnership to Fight Chronic DiseaseBelum ada peringkat
- Covered California: Expanding Coverage, Promoting Value and Supporting At-Risk EnrolleesDokumen25 halamanCovered California: Expanding Coverage, Promoting Value and Supporting At-Risk EnrolleesPartnership to Fight Chronic DiseaseBelum ada peringkat
- Project Data SphereDokumen1 halamanProject Data SpherePartnership to Fight Chronic DiseaseBelum ada peringkat
- About Caregiver Action NetworkDokumen1 halamanAbout Caregiver Action NetworkPartnership to Fight Chronic DiseaseBelum ada peringkat
- Effective Approaches For Managing Obesity and Chronic DiseaseDokumen18 halamanEffective Approaches For Managing Obesity and Chronic DiseasePartnership to Fight Chronic DiseaseBelum ada peringkat
- The Power of Partnerships - The Bulgarian National Patients' OrganizationDokumen19 halamanThe Power of Partnerships - The Bulgarian National Patients' OrganizationPartnership to Fight Chronic DiseaseBelum ada peringkat
- National Family Caregivers MonthDokumen1 halamanNational Family Caregivers MonthPartnership to Fight Chronic DiseaseBelum ada peringkat
- A Short Introduction To Future Approaches in Chronic DiseasesDokumen30 halamanA Short Introduction To Future Approaches in Chronic DiseasesPartnership to Fight Chronic DiseaseBelum ada peringkat
- Facilitating Patient Advocacy Expertise Across BordersDokumen9 halamanFacilitating Patient Advocacy Expertise Across BordersPartnership to Fight Chronic DiseaseBelum ada peringkat
- Fighting Chronic Disease: The Power of PartnershipDokumen25 halamanFighting Chronic Disease: The Power of PartnershipPartnership to Fight Chronic DiseaseBelum ada peringkat
- Tatar - Non Communicable Diseases enDokumen28 halamanTatar - Non Communicable Diseases enPartnership to Fight Chronic DiseaseBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Manual On Cargo Clearance Process (E2m Customs Import Assessment System)Dokumen43 halamanManual On Cargo Clearance Process (E2m Customs Import Assessment System)Musa Batugan Jr.100% (1)
- MOTORESDokumen6 halamanMOTORESAlberto Israel MartínezBelum ada peringkat
- Xeridt2n cbn9637661Dokumen7 halamanXeridt2n cbn9637661Naila AshrafBelum ada peringkat
- Terminal Injustice - Ambush AttackDokumen2 halamanTerminal Injustice - Ambush AttackAllen Carlton Jr.Belum ada peringkat
- Pathwinder Software v. Core Cashless - Personal Jurisdiction PDFDokumen19 halamanPathwinder Software v. Core Cashless - Personal Jurisdiction PDFMark JaffeBelum ada peringkat
- CentipedeDokumen2 halamanCentipedeMaeBelum ada peringkat
- Gabriel Marcel - Sketch of A Phenomenology and A Metaphysic of HopeDokumen6 halamanGabriel Marcel - Sketch of A Phenomenology and A Metaphysic of HopeHazel Dawn PaticaBelum ada peringkat
- Nittscher vs. NittscherDokumen4 halamanNittscher vs. NittscherKeej DalonosBelum ada peringkat
- سلفات بحري كومنز PDFDokumen8 halamanسلفات بحري كومنز PDFSami KahtaniBelum ada peringkat
- What Is Supply Chain ManagementDokumen3 halamanWhat Is Supply Chain ManagementozkanyilmazBelum ada peringkat
- Machiavellian Thinking vs. Conventional Logic - Illimitable MenDokumen16 halamanMachiavellian Thinking vs. Conventional Logic - Illimitable MenMaurice BathichBelum ada peringkat
- Denial of Right Warning of Arrest Intent To Lien Affidavit of Complaint Walmart GM Lee Store #2360 in Play Time Is Over The TruthDokumen11 halamanDenial of Right Warning of Arrest Intent To Lien Affidavit of Complaint Walmart GM Lee Store #2360 in Play Time Is Over The Truthahmal coaxumBelum ada peringkat
- Physics Project Work Part 2Dokumen9 halamanPhysics Project Work Part 2Find LetBelum ada peringkat
- Acts and Key EventsDokumen25 halamanActs and Key Eventsemilyjaneboyle100% (1)
- 2022 - Notice - Bill of Particulars DemandDokumen5 halaman2022 - Notice - Bill of Particulars DemandbrandonBelum ada peringkat
- Retrato Alvin YapanDokumen8 halamanRetrato Alvin YapanAngel Jan AgpalzaBelum ada peringkat
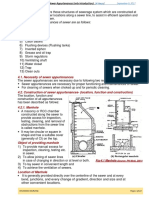
- Unit-4 Sewer Appurtenances - Only Introduction (4 Hours) R2Dokumen13 halamanUnit-4 Sewer Appurtenances - Only Introduction (4 Hours) R2Girman RanaBelum ada peringkat
- Quiz 5Dokumen5 halamanQuiz 5asaad5299Belum ada peringkat
- Java Heritage Hotel ReportDokumen11 halamanJava Heritage Hotel ReportنصرالحكمالغزلىBelum ada peringkat
- 2020 2021 Important JudgementsDokumen6 halaman2020 2021 Important JudgementsRidam Saini100% (1)
- Mollymawk - English (Çalışma)Dokumen8 halamanMollymawk - English (Çalışma)Fatih OguzBelum ada peringkat
- Policies Toward Monopolies and Oligopolies Privatization and DeregulationDokumen10 halamanPolicies Toward Monopolies and Oligopolies Privatization and DeregulationJamaica RamosBelum ada peringkat
- ET Banking & FinanceDokumen35 halamanET Banking & FinanceSunchit SethiBelum ada peringkat
- CRM AssignmentDokumen43 halamanCRM Assignmentharshdeep mehta100% (2)
- Unit 1 - IntroductionDokumen15 halamanUnit 1 - IntroductionJorge Martínez SáinzBelum ada peringkat
- Marudur,+6 +nikaDokumen12 halamanMarudur,+6 +nikaResandi MuhamadBelum ada peringkat
- CASE DOCTRINE FDokumen17 halamanCASE DOCTRINE FKaemy MalloBelum ada peringkat
- COWASH Federal Admin Manual v11 PDFDokumen26 halamanCOWASH Federal Admin Manual v11 PDFmaleriBelum ada peringkat
- Ch02 Choice in World of ScarcityDokumen14 halamanCh02 Choice in World of ScarcitydankBelum ada peringkat
- JoB Details & Description Interns For ARISTA VAULTDokumen7 halamanJoB Details & Description Interns For ARISTA VAULTDisha KesarwaniBelum ada peringkat