Anda mungkin juga menyukai
- Hair Loss SecretsDokumen81 halamanHair Loss SecretsUtkarsh100% (1)
- 3 Massive Mistakes 10 29 15 Slide DeckDokumen76 halaman3 Massive Mistakes 10 29 15 Slide DeckemagooBelum ada peringkat
- Enhanced Growth of The Adult Penis With Vitamin D 3: January 2009Dokumen9 halamanEnhanced Growth of The Adult Penis With Vitamin D 3: January 2009WhiteBelum ada peringkat
- How To Increase Libido The Natural WayDokumen8 halamanHow To Increase Libido The Natural Waypaul macharia100% (1)
- 10 Steps To Get Out of Debt and Start Saving Ebook 2018.03 - Fa LRDokumen68 halaman10 Steps To Get Out of Debt and Start Saving Ebook 2018.03 - Fa LRTamer FawzyBelum ada peringkat
- How To Market Your MusicDokumen12 halamanHow To Market Your MusicyoutubeseoexpertBelum ada peringkat
- 8 Proven Ways To Increase Testosterone Levels NaturallyDokumen6 halaman8 Proven Ways To Increase Testosterone Levels Naturallymartinscribd7Belum ada peringkat
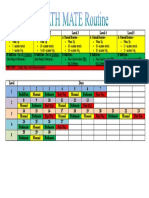
- Day 1 (Bathmate and Extender Day) Day 7 (Rest Day) : The RoutineDokumen2 halamanDay 1 (Bathmate and Extender Day) Day 7 (Rest Day) : The RoutineRien Jing TianBelum ada peringkat
- Andrew Tate Net WorthDokumen3 halamanAndrew Tate Net Worthواجد چوھدریBelum ada peringkat
- Principles 101Dokumen291 halamanPrinciples 101evilvalleBelum ada peringkat
- Men's Formula For Prostate Health & General Well-BeingDokumen18 halamanMen's Formula For Prostate Health & General Well-BeingFnnewsBelum ada peringkat
- BATHMATE RoutineDokumen1 halamanBATHMATE RoutineRien Jing TianBelum ada peringkat
- Imaging Anatomy Brain and Spine Osborn 1 Ed 2020 PDFDokumen3.130 halamanImaging Anatomy Brain and Spine Osborn 1 Ed 2020 PDFthe gaangster100% (1)
- Bonus Recipe Sexual SurgeDokumen5 halamanBonus Recipe Sexual Surgebujor2000aja100% (1)
- Sex Drive Tips Design MMDokumen50 halamanSex Drive Tips Design MMMustafa JimaleBelum ada peringkat
- Mind Hacking With Sir John H.. - BrainfluencePodcDokumen22 halamanMind Hacking With Sir John H.. - BrainfluencePodcLazlo SecretBelum ada peringkat
- Meditation: The Meditation Guide for a Peaceful and Stress-Free LifeDari EverandMeditation: The Meditation Guide for a Peaceful and Stress-Free LifeBelum ada peringkat
- Local Birthday Leads Training Manual RevisedDokumen49 halamanLocal Birthday Leads Training Manual RevisedpdkonlineBelum ada peringkat
- Biological ExerciseDokumen6 halamanBiological ExerciseTanmoy BasakBelum ada peringkat
- Clear SkinDokumen66 halamanClear SkinalouisBelum ada peringkat
- Mens Clinic TRT ReplacementDokumen9 halamanMens Clinic TRT ReplacementMikey FurrowBelum ada peringkat
- Full Download Bontragers Textbook of Radiographic Positioning and Related Anatomy 9th Edition Lampignano Test BankDokumen36 halamanFull Download Bontragers Textbook of Radiographic Positioning and Related Anatomy 9th Edition Lampignano Test Bankjohn5kwillis100% (22)
- How To Naturally Increase TestosteroneDokumen149 halamanHow To Naturally Increase TestosteronePádraig Mag FhionnghaileBelum ada peringkat
- Primal Grow ProDokumen4 halamanPrimal Grow ProSarah SmithBelum ada peringkat
- Alongamento Do Pénis em Pacientes Que Têm HipogonadismoDokumen1 halamanAlongamento Do Pénis em Pacientes Que Têm Hipogonadismovacextensor1050% (2)
- Metabolic Cooking PDF, Ebook by Karen Losier and Dave RuelDokumen16 halamanMetabolic Cooking PDF, Ebook by Karen Losier and Dave RuelNatalie WalkerBelum ada peringkat
- Living to 120 and Beyond: Where Science and Spirit MeetDari EverandLiving to 120 and Beyond: Where Science and Spirit MeetBelum ada peringkat
- A Historical Analysis of Inernational Inclusive Education Policy With DisabilitiesDokumen12 halamanA Historical Analysis of Inernational Inclusive Education Policy With DisabilitiesYugesh D PANDAYBelum ada peringkat
- LeverFrederickPeplau 2006PMM PenisSizeSatisfactionDokumen15 halamanLeverFrederickPeplau 2006PMM PenisSizeSatisfactionacer551Belum ada peringkat
- Male vs. Female Depression: Why Men Act Out and Women Act inDokumen18 halamanMale vs. Female Depression: Why Men Act Out and Women Act inJed Diamond100% (9)
- Andrew Tate Is Banned From Social Media Platforms NPRDokumen1 halamanAndrew Tate Is Banned From Social Media Platforms NPRfBelum ada peringkat
- How To Increase Your Testosterone NaturallyDokumen2 halamanHow To Increase Your Testosterone NaturallyJohn YeoBelum ada peringkat
- Best Natural Work Male EnhancementDokumen9 halamanBest Natural Work Male EnhancementAndrewJonathanBelum ada peringkat
- Ejaculation ProblemDokumen4 halamanEjaculation ProblemYaho HosBelum ada peringkat
- The Gender Spectrum - A Scientist Explains Why Gender Isn't BinaryDokumen16 halamanThe Gender Spectrum - A Scientist Explains Why Gender Isn't BinaryTokiyo LanfrancoBelum ada peringkat
- Struktur Lipid - SteroidDokumen8 halamanStruktur Lipid - SteroidRisyad NaufalBelum ada peringkat
- Promtional Events for Bars, Nightclubs and Strip ClubsDari EverandPromtional Events for Bars, Nightclubs and Strip ClubsBelum ada peringkat
- Sextasy 101: The Ultimate Guide for Relationships and Sex On XDari EverandSextasy 101: The Ultimate Guide for Relationships and Sex On XBelum ada peringkat
- Ancient To Roman EducationDokumen10 halamanAncient To Roman EducationAnonymous wwq9kKDY4100% (2)
- Ton Miles Calculation 1Dokumen17 halamanTon Miles Calculation 1Alexander Armando Clemente Andrade100% (1)
- VRealize Operations Manager Installation and Configuration Guide For Linux and WindowsDokumen98 halamanVRealize Operations Manager Installation and Configuration Guide For Linux and Windowsamdusias67Belum ada peringkat
- 50 Fitness Myths: Don't Believe All the HypeDari Everand50 Fitness Myths: Don't Believe All the HypePenilaian: 3 dari 5 bintang3/5 (1)
- X RunnerDokumen24 halamanX RunnerJack MaBelum ada peringkat
- Anatomy of PenisDokumen30 halamanAnatomy of PenisKousik AmancharlaBelum ada peringkat
- CC June 2013 PDFDokumen9 halamanCC June 2013 PDFemagooBelum ada peringkat
- Body Image Dissatisfaction: Gender Differences in Eating Attitudes, Self-Esteem, and Reasons For ExerciseDokumen18 halamanBody Image Dissatisfaction: Gender Differences in Eating Attitudes, Self-Esteem, and Reasons For ExerciseNimic NimicBelum ada peringkat
- Can Oral Sex Transmit HIV?Dokumen52 halamanCan Oral Sex Transmit HIV?Leo LamsBelum ada peringkat
- How To Woo A Woman: How To Find,Date And Marry The Woman Of Your DreamsDari EverandHow To Woo A Woman: How To Find,Date And Marry The Woman Of Your DreamsBelum ada peringkat
- 40 Irresistible First Date IdeasDokumen44 halaman40 Irresistible First Date IdeasAbhayBelum ada peringkat
- PenisDokumen2 halamanPenismichelle labaoBelum ada peringkat
- Solution To Youh's Problem by Asghar Ali ChowdharyDokumen81 halamanSolution To Youh's Problem by Asghar Ali Chowdharyfar_bhatti8029100% (1)
- Make The Most of Better in Bed by Adam Armstrong Review EbooksDokumen1 halamanMake The Most of Better in Bed by Adam Armstrong Review EbooksNaison StanleyBelum ada peringkat
- You Don’t Have to Be a Champion... to Be a Winner!: A journey from Xerox to F1Dari EverandYou Don’t Have to Be a Champion... to Be a Winner!: A journey from Xerox to F1Belum ada peringkat
- Ways To Drive Traffic: To Your Medspa WebsiteDokumen20 halamanWays To Drive Traffic: To Your Medspa WebsiteSIDDHESH WADEKARBelum ada peringkat
- Anti-Aging Medicine 777Dokumen114 halamanAnti-Aging Medicine 777Kiné Therapeut-manuelle Masseur GabiBelum ada peringkat
- Consumer Buying Behavior Towards Toothpaste Brands in Ludhiana"Dokumen43 halamanConsumer Buying Behavior Towards Toothpaste Brands in Ludhiana"Amit Attri33% (3)
- Entrepreneurial SellingDokumen24 halamanEntrepreneurial SellingCharleneKronstedtBelum ada peringkat
- If You Don’t Ask The Answer Is No: A Practical Guide for Getting Through College Without Falling Through the CracksDari EverandIf You Don’t Ask The Answer Is No: A Practical Guide for Getting Through College Without Falling Through the CracksBelum ada peringkat
- Value From Hedonic Experience and EngagementDokumen22 halamanValue From Hedonic Experience and EngagementYugesh D PANDAYBelum ada peringkat
- When Passion Makes The Heart Grow Colder: The Role of Passion in Alternative Goal SuppressionDokumen22 halamanWhen Passion Makes The Heart Grow Colder: The Role of Passion in Alternative Goal SuppressionYugesh D PANDAYBelum ada peringkat
- Main Art CielDokumen12 halamanMain Art CielSunil KumarBelum ada peringkat
- Executive Coaching It WorksDokumen13 halamanExecutive Coaching It WorksCarlos Farfan CalderonBelum ada peringkat
- Action Plan For Partriotic EducationDokumen13 halamanAction Plan For Partriotic EducationYugesh D PANDAYBelum ada peringkat
- Are You Leading, or Just Managing To Get By?Dokumen5 halamanAre You Leading, or Just Managing To Get By?Yugesh D PANDAYBelum ada peringkat
- Nature's Clocks and Human Mood: The Circadian System Modulates Reward MotivationDokumen12 halamanNature's Clocks and Human Mood: The Circadian System Modulates Reward MotivationYugesh D PANDAYBelum ada peringkat
- Impact of Feedback On Goal Setting and Task PerformanceDokumen11 halamanImpact of Feedback On Goal Setting and Task PerformanceYugesh D PANDAYBelum ada peringkat
- Human Capital EntrpreneHuman Capital, Migration and Rural Entrepreneurship in Chinaurship in Rural ChinaDokumen23 halamanHuman Capital EntrpreneHuman Capital, Migration and Rural Entrepreneurship in Chinaurship in Rural ChinaYugesh D PANDAYBelum ada peringkat
- Implicit Motives Explicit TraitsDokumen17 halamanImplicit Motives Explicit TraitsYugesh D PANDAYBelum ada peringkat
- Civic Education Reform in Taiwan: Directions, Controversies, and ChallengesDokumen13 halamanCivic Education Reform in Taiwan: Directions, Controversies, and ChallengesYugesh D PANDAYBelum ada peringkat
- Empowering Leaders Optimize Working Conditions For Engagement: A Multilevel StudyDokumen13 halamanEmpowering Leaders Optimize Working Conditions For Engagement: A Multilevel StudyYugesh D PANDAYBelum ada peringkat
- Chinese Ed System Past PresSleeping Giant: Chinese Teacher Education System Past, Present and Future (I) Ent FutureDokumen6 halamanChinese Ed System Past PresSleeping Giant: Chinese Teacher Education System Past, Present and Future (I) Ent FutureYugesh D PANDAYBelum ada peringkat
- Emotional Intelligence and Leadership in AdolescentsDokumen13 halamanEmotional Intelligence and Leadership in AdolescentsYugesh D PANDAYBelum ada peringkat
- Curriculum Making For China'Dokumen2 halamanCurriculum Making For China'Yugesh D PANDAYBelum ada peringkat
- Perceived Social Change and Childrearing Attitudes in ChinaDokumen11 halamanPerceived Social Change and Childrearing Attitudes in ChinaYugesh D PANDAYBelum ada peringkat
- Analysis On Inter-Provincial Disparities of China's Rural Education and Convergence Rate Empirical Analysis On 31 Provinces' (Municipalities') Panel Data From 2001 To 2008Dokumen10 halamanAnalysis On Inter-Provincial Disparities of China's Rural Education and Convergence Rate Empirical Analysis On 31 Provinces' (Municipalities') Panel Data From 2001 To 2008Yugesh D PANDAYBelum ada peringkat
- Are You Leading, or Just Managing To Get By?Dokumen5 halamanAre You Leading, or Just Managing To Get By?Yugesh D PANDAYBelum ada peringkat
- Education System Reform in China After 1978: Some Practical ImplicationsDokumen16 halamanEducation System Reform in China After 1978: Some Practical ImplicationsYugesh D PANDAYBelum ada peringkat
- TRIAGRAM: A Gifted and Talented Educational Programme That All Students Can EnjoyDokumen5 halamanTRIAGRAM: A Gifted and Talented Educational Programme That All Students Can EnjoyYugesh D PANDAYBelum ada peringkat
- Using Mixed Methods in Monitoring and Evaluation Experiences From International DevelopmentDokumen30 halamanUsing Mixed Methods in Monitoring and Evaluation Experiences From International DevelopmentYugesh D PANDAYBelum ada peringkat
- Underestimating Youth's Commitment To Schools and Society: Toward A More Differentiated ViewDokumen40 halamanUnderestimating Youth's Commitment To Schools and Society: Toward A More Differentiated ViewYugesh D PANDAYBelum ada peringkat
- Motivator and Hygiene Dimensions For Research and Development Engineers1Dokumen4 halamanMotivator and Hygiene Dimensions For Research and Development Engineers1Yugesh D PANDAYBelum ada peringkat
- The Man Who Said He Was GodDokumen2 halamanThe Man Who Said He Was GodYugesh D PANDAYBelum ada peringkat
- A Blueprint For Reform - Obama Proposed Educatioanl ReformDokumen45 halamanA Blueprint For Reform - Obama Proposed Educatioanl ReformYugesh D PANDAYBelum ada peringkat
- Psychology of Man and MasculinityDokumen16 halamanPsychology of Man and MasculinityYugesh D PANDAYBelum ada peringkat
- Achievement Goals As Predictors of Achievement-Relevant Processes Prior To Task EngagementDokumen15 halamanAchievement Goals As Predictors of Achievement-Relevant Processes Prior To Task EngagementYugesh D PANDAYBelum ada peringkat
- Educational & Human Resource Strategic Plan 2008-2020Dokumen164 halamanEducational & Human Resource Strategic Plan 2008-2020Yugesh D PANDAYBelum ada peringkat
- Evaluation of Teacher Appraisal in A SchoolDokumen8 halamanEvaluation of Teacher Appraisal in A SchoolYugesh D PANDAYBelum ada peringkat
- Lifecycle of A Frog For Primary StudentsDokumen10 halamanLifecycle of A Frog For Primary StudentsMónika KissBelum ada peringkat
- Probset 3 KeyDokumen7 halamanProbset 3 KeyhoneyschuBelum ada peringkat
- CD4 12-P374493Dokumen30 halamanCD4 12-P374493suraj_savant1Belum ada peringkat
- Operation Manual-KINGSTONE SDP-ENG-20120205 PDFDokumen49 halamanOperation Manual-KINGSTONE SDP-ENG-20120205 PDFJiménezBelum ada peringkat
- Prevention of Power Theft Using Concept of Multifunction Meter and PLCDokumen6 halamanPrevention of Power Theft Using Concept of Multifunction Meter and PLCMuhammad FarhanBelum ada peringkat
- R917007195 Comando 8RDokumen50 halamanR917007195 Comando 8RRodrigues de OliveiraBelum ada peringkat
- Fisker Karma - Battery 12V Jump StartDokumen2 halamanFisker Karma - Battery 12V Jump StartRedacTHORBelum ada peringkat
- Topic - Temperature SensorDokumen9 halamanTopic - Temperature SensorSaloni ChaudharyBelum ada peringkat
- School of Management Studies INDIRA GANDHI NATIONAL OPEN UNIVERSITY Proforma For Approval of Project Proposal (MS-100)Dokumen12 halamanSchool of Management Studies INDIRA GANDHI NATIONAL OPEN UNIVERSITY Proforma For Approval of Project Proposal (MS-100)Pramod ShawBelum ada peringkat
- ActivityDokumen2 halamanActivityShaira May SalvadorBelum ada peringkat
- An Overview of Marketing - Week 1Dokumen7 halamanAn Overview of Marketing - Week 1Jowjie TVBelum ada peringkat
- Job Stress InterventionsDokumen5 halamanJob Stress InterventionscocaralucamihaelaBelum ada peringkat
- New Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)Dokumen42 halamanNew Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)stan.isgod99Belum ada peringkat
- Operaciones UnitariasDokumen91 halamanOperaciones UnitariasAlejandro ReyesBelum ada peringkat
- Dial 1298 For Ambulance - HSBCDokumen22 halamanDial 1298 For Ambulance - HSBCDial1298forAmbulanceBelum ada peringkat
- MGN815: Business Models: Ajay ChandelDokumen38 halamanMGN815: Business Models: Ajay ChandelSam RehmanBelum ada peringkat
- Ahu 1997 22 1 95Dokumen15 halamanAhu 1997 22 1 95Pasajera En TranceBelum ada peringkat
- Faculty of Engineering & TechnologyDokumen15 halamanFaculty of Engineering & TechnologyGangu VirinchiBelum ada peringkat
- The Eye WorksheetDokumen3 halamanThe Eye WorksheetCally ChewBelum ada peringkat
- Poster PresentationDokumen3 halamanPoster PresentationNipun RavalBelum ada peringkat
- Second Language Learning in The Classroom PDFDokumen2 halamanSecond Language Learning in The Classroom PDFThanh Phương VõBelum ada peringkat
- Practice Paper Pre Board Xii Biology 2023-24-1Dokumen6 halamanPractice Paper Pre Board Xii Biology 2023-24-1salamnaseema14Belum ada peringkat
- Grade 8 Science Text Book 61fb9947be91fDokumen289 halamanGrade 8 Science Text Book 61fb9947be91fNadarajah PragatheeswarBelum ada peringkat
- Benefits and Drawbacks of Thermal Pre-Hydrolysis For Operational Performance of Wastewater Treatment PlantsDokumen7 halamanBenefits and Drawbacks of Thermal Pre-Hydrolysis For Operational Performance of Wastewater Treatment PlantsmartafhBelum ada peringkat
- Annexure To SOW 3 STD Specification For Welding and NDT PipingDokumen15 halamanAnnexure To SOW 3 STD Specification For Welding and NDT PipingASHISH GORDEBelum ada peringkat