Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Clerkship ManualDokumen19 halamanClerkship ManualVanessa Marie Ty Lim100% (2)
- Myers CocktailDokumen15 halamanMyers CocktailViladosgirassois Couto PinonBelum ada peringkat
- Molar Uprighting / Orthodontic Courses by Indian Dental AcademyDokumen142 halamanMolar Uprighting / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Diabetic FootDokumen46 halamanDiabetic FootRhapsody RedBelum ada peringkat
- Oxygen Administration ChecklistDokumen2 halamanOxygen Administration ChecklistCamacho, Aronne Eoin A.100% (3)
- ObturatorsDokumen79 halamanObturatorsPremshith CpBelum ada peringkat
- The Recent History of AcupunctureDokumen2 halamanThe Recent History of AcupunctureBhaskaranBelum ada peringkat
- Active Ingredients Used in Cosmetics: Safety SurveyDokumen2 halamanActive Ingredients Used in Cosmetics: Safety SurveyCouncil of Europe67% (3)
- NEMBY Jr. Schedule June, 2014Dokumen1 halamanNEMBY Jr. Schedule June, 2014Mark DurksenBelum ada peringkat
- NEMBY Jr. Swimming FormDokumen1 halamanNEMBY Jr. Swimming FormMark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Calendar (2014-04)Dokumen1 halamanNEMBY Jr. Monthly Calendar (2014-04)Mark DurksenBelum ada peringkat
- NEMBY Jr. Bowling FormDokumen1 halamanNEMBY Jr. Bowling FormMark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Calendar (2014-03)Dokumen1 halamanNEMBY Jr. Monthly Calendar (2014-03)Mark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Schedule (2013-10)Dokumen1 halamanNEMBY Jr. Monthly Schedule (2013-10)Mark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Schedule 2013-11Dokumen1 halamanNEMBY Jr. Monthly Schedule 2013-11Mark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Calendar (2014-02)Dokumen1 halamanNEMBY Jr. Monthly Calendar (2014-02)Mark DurksenBelum ada peringkat
- Deep Freeze 2014 Camp Permission FormDokumen1 halamanDeep Freeze 2014 Camp Permission FormMark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Schedule (2013-09)Dokumen1 halamanNEMBY Jr. Monthly Schedule (2013-09)Mark DurksenBelum ada peringkat
- What Is Deep Freeze?: Thursday, Dec. 20 - If You've Got Any Questions Call Mark or Sabrina atDokumen4 halamanWhat Is Deep Freeze?: Thursday, Dec. 20 - If You've Got Any Questions Call Mark or Sabrina atMark DurksenBelum ada peringkat
- NEMBY Jr. Blue Jays FormDokumen2 halamanNEMBY Jr. Blue Jays FormMark DurksenBelum ada peringkat
- NEMBY Jr. Port Dalhousie FormDokumen1 halamanNEMBY Jr. Port Dalhousie FormMark DurksenBelum ada peringkat
- NEMBY Jr. Pool Party FormDokumen1 halamanNEMBY Jr. Pool Party FormMark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Schedule (2013-03)Dokumen1 halamanNEMBY Jr. Monthly Schedule (2013-03)Mark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Schedul (2013-05)Dokumen1 halamanNEMBY Jr. Monthly Schedul (2013-05)Mark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Schedule (2013/01)Dokumen1 halamanNEMBY Jr. Monthly Schedule (2013/01)Mark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Schedule (2012/11)Dokumen1 halamanNEMBY Jr. Monthly Schedule (2012/11)Mark DurksenBelum ada peringkat
- NEMBY Jr. Monthly Schedule (2012/10)Dokumen1 halamanNEMBY Jr. Monthly Schedule (2012/10)Mark DurksenBelum ada peringkat
- Call To Action On NCDS: Challenges and Way Forward For Maternal and Child HealthDokumen32 halamanCall To Action On NCDS: Challenges and Way Forward For Maternal and Child HealthSadi KhanBelum ada peringkat
- Ebola Virus Disease (WHO) : Key FactsDokumen5 halamanEbola Virus Disease (WHO) : Key FactsridhosetyawanBelum ada peringkat
- RRL LucmanDokumen2 halamanRRL LucmanNor-hayne LucmanBelum ada peringkat
- The US Pharmacy Benefit Management (PBM) Industry Report: 2013 Edition - New Report by Koncept AnalyticsDokumen10 halamanThe US Pharmacy Benefit Management (PBM) Industry Report: 2013 Edition - New Report by Koncept AnalyticsKoncept AnalyticsBelum ada peringkat
- Referral Slip - Antel Holdings, EditedDokumen1 halamanReferral Slip - Antel Holdings, EditedDth MonisBelum ada peringkat
- Adherence To Cardiovascular Therapy: A Meta-Analysis of Prevalence and Clinical ConsequencesDokumen9 halamanAdherence To Cardiovascular Therapy: A Meta-Analysis of Prevalence and Clinical Consequencesdaniela NeculmanBelum ada peringkat
- MID1112ra DavaoDokumen32 halamanMID1112ra DavaoNonoyTaclinoBelum ada peringkat
- Forcep DeliveryDokumen32 halamanForcep DeliverybbaltazarjaniceBelum ada peringkat
- jURNAL Anc tERPADUDokumen8 halamanjURNAL Anc tERPADUcathyBelum ada peringkat
- Essential Components of Primary Eye Care: EditorialDokumen3 halamanEssential Components of Primary Eye Care: EditorialAreenaBelum ada peringkat
- Acute PancreatitisDokumen7 halamanAcute PancreatitisVytheeshwaran Vedagiri100% (9)
- JMS 119 - EKG Dasar - NZ Edited 2018Dokumen41 halamanJMS 119 - EKG Dasar - NZ Edited 2018Cindy RiannieBelum ada peringkat
- Infant MMDST AssessmentDokumen36 halamanInfant MMDST AssessmentLai KuanlinBelum ada peringkat
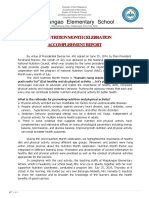
- Narrative Report 2019mDokumen10 halamanNarrative Report 2019mCcatherine Isanan-HilisanBelum ada peringkat
- Karwatzky ActivatorDokumen8 halamanKarwatzky ActivatorSankhyaBelum ada peringkat
- Chapter 14Dokumen4 halamanChapter 14Allynne Jane DagasdasBelum ada peringkat
- Clustering Data Sheet and Concept Map and Nursing Care Plan HTNDokumen4 halamanClustering Data Sheet and Concept Map and Nursing Care Plan HTNAyman NabilBelum ada peringkat
- Program EssayDokumen2 halamanProgram Essaymacey wardBelum ada peringkat
- RCT - Masters - 2022Dokumen24 halamanRCT - Masters - 2022Kanwal KhanBelum ada peringkat
- PhRMA Marketing Brochure Influences On Prescribing FINALDokumen12 halamanPhRMA Marketing Brochure Influences On Prescribing FINALJalwaz TihamiBelum ada peringkat
- PANR Part 1Dokumen2 halamanPANR Part 1Jastine SabornidoBelum ada peringkat
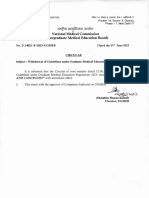
- RRQRQ: 3ttgffihrr National Medical Medical EducationDokumen2 halamanRRQRQ: 3ttgffihrr National Medical Medical EducationF LalramluahpuiaBelum ada peringkat