Anda mungkin juga menyukai
- OR 01a FCDokumen12 halamanOR 01a FCfritzrose50% (2)
- Acid-Base WorksheetDokumen2 halamanAcid-Base WorksheetMayer Rosenberg100% (18)
- Assignment 4Dokumen8 halamanAssignment 4api-328441669100% (1)
- Simple Method of Acid Base Balance InterpretationDokumen11 halamanSimple Method of Acid Base Balance InterpretationChin ChanBelum ada peringkat
- Respiratory FailureDokumen7 halamanRespiratory FailuremuhammadridhwanBelum ada peringkat
- Arterial Blood GasDokumen55 halamanArterial Blood GasRathis Dasan100% (1)
- Easy Way To Interpret ABG ValuesDokumen7 halamanEasy Way To Interpret ABG ValuesDoyTanBelum ada peringkat
- Metabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandMetabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Arterial Blood Gas Values Case Study 2Dokumen3 halamanArterial Blood Gas Values Case Study 2julissaBelum ada peringkat
- Arterialbloodgasanalysis ppt-2Dokumen43 halamanArterialbloodgasanalysis ppt-2Kresna Dharma SuryanaBelum ada peringkat
- Case Histo PDFDokumen19 halamanCase Histo PDFsomayya waliBelum ada peringkat
- Oxygen Therapy: Housemanship Training Programme Department of Anaesthesiology and Intensive CareDokumen55 halamanOxygen Therapy: Housemanship Training Programme Department of Anaesthesiology and Intensive CaretorreslysBelum ada peringkat
- Renal DialysisDokumen14 halamanRenal Dialysisjhodane100% (1)
- ARDS CaseStudy BDokumen7 halamanARDS CaseStudy BCORROS JASMIN MARIEBelum ada peringkat
- Impaired Gas ExchangeDokumen4 halamanImpaired Gas ExchangeNuraini Hamzah100% (1)
- Critical Care Alterations in RespiratoryDokumen96 halamanCritical Care Alterations in RespiratoryNatukunda DianahBelum ada peringkat
- Nursing Care of Clients With Upper Gastrointestinal Disorder 1Dokumen149 halamanNursing Care of Clients With Upper Gastrointestinal Disorder 1Andrea TylerBelum ada peringkat
- Fluids and ElectrolytesDokumen192 halamanFluids and ElectrolytesTeodora JoghiuBelum ada peringkat
- Fluid and Electrolyte Imbalance QuizDokumen2 halamanFluid and Electrolyte Imbalance QuizteabagmanBelum ada peringkat
- Thesis 2Dokumen70 halamanThesis 2Angeline Alpure MoralesBelum ada peringkat
- NocturiaDokumen10 halamanNocturiaKousik AmancharlaBelum ada peringkat
- Diarrhea: Persistent If 2-4 Weeks, and Chronic If 4 Weeks in DurationDokumen12 halamanDiarrhea: Persistent If 2-4 Weeks, and Chronic If 4 Weeks in DurationAnonymous IWRTYznDZnBelum ada peringkat
- ABG QuizDokumen3 halamanABG QuizMelchor Felipe SalvosaBelum ada peringkat
- Abg AnalysisDokumen65 halamanAbg AnalysisSyed Farooque AliBelum ada peringkat
- Arterial Blood Gas: Collection and InterpretationDokumen23 halamanArterial Blood Gas: Collection and InterpretationJellyAnnAujeroSanchez100% (1)
- Febuxostat (Uloric), A New Treatment Option For Gout: Carmela Avena-Woods Olga Hilas Author Information Go ToDokumen9 halamanFebuxostat (Uloric), A New Treatment Option For Gout: Carmela Avena-Woods Olga Hilas Author Information Go ToAnadi GuptaBelum ada peringkat
- Acid-Base Disorder 27 July 2017 PDFDokumen48 halamanAcid-Base Disorder 27 July 2017 PDFPauline ChanBelum ada peringkat
- Body Fluid DistributionDokumen56 halamanBody Fluid DistributionZoya Morani100% (1)
- Interpretation of Results ReportingDokumen7 halamanInterpretation of Results ReportingMerill Harrelson LibanBelum ada peringkat
- Pleural Fluid AnalysisDokumen15 halamanPleural Fluid AnalysisNatalie Sarah MoonBelum ada peringkat
- Hypoxia and CyanosisDokumen33 halamanHypoxia and CyanosisRamlah IbrahimBelum ada peringkat
- Chronic Obstructive Pulnonary Disease (Copd)Dokumen3 halamanChronic Obstructive Pulnonary Disease (Copd)Richard TanBelum ada peringkat
- Ebp PaperDokumen8 halamanEbp Paperapi-250304529Belum ada peringkat
- 5 FMCH Research BiasDokumen3 halaman5 FMCH Research BiasMia CadizBelum ada peringkat
- Abg InterpretationDokumen13 halamanAbg Interpretationgwapz23Belum ada peringkat
- Addison and Cushing DMDokumen22 halamanAddison and Cushing DManon_391984943Belum ada peringkat
- M1 - ABG InterpretDokumen2 halamanM1 - ABG InterpretjuiceBelum ada peringkat
- Acid Base DisordersDokumen5 halamanAcid Base DisordersjohnshenryBelum ada peringkat
- Renal Failure PresentationDokumen65 halamanRenal Failure PresentationBhawna JoshiBelum ada peringkat
- 406 - Respiratory Therapy Consult Service HandbookDokumen28 halaman406 - Respiratory Therapy Consult Service HandbookIkhsan JohnsonBelum ada peringkat
- PHARMACOLOGY - Midterms 1.6-Fluid and Electrolyte TRANSDokumen13 halamanPHARMACOLOGY - Midterms 1.6-Fluid and Electrolyte TRANSNooneBelum ada peringkat
- Fluid Balance in Clinical PracticeDokumen8 halamanFluid Balance in Clinical Practicefernando_vaz2010100% (1)
- Congestive Heart FailureDokumen14 halamanCongestive Heart FailureBella Trix PagdangananBelum ada peringkat
- ABG InterpretationDokumen10 halamanABG InterpretationNisha MathewBelum ada peringkat
- Cervical CA Case StudyDokumen32 halamanCervical CA Case StudyCandy Mae Kabayao CuraBelum ada peringkat
- Burns Pathophysiology 2Dokumen1 halamanBurns Pathophysiology 2Monique Ann DanoyBelum ada peringkat
- Nursing Process Diagnosis Plan Implementation EvaluationDokumen59 halamanNursing Process Diagnosis Plan Implementation EvaluationYemaya84Belum ada peringkat
- Pediatrics Block 2Dokumen207 halamanPediatrics Block 2Ghada ElhassanBelum ada peringkat
- Blood and Blood Components-LectureDokumen12 halamanBlood and Blood Components-LectureSj EclipseBelum ada peringkat
- IV Infusion SolutionDokumen8 halamanIV Infusion SolutionmohammedBelum ada peringkat
- Adults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofDokumen2 halamanAdults With Suspected Epiglottitis - Supraglottitis Guidelines For The Management ofAlexandros MegasBelum ada peringkat
- DARDokumen4 halamanDARfritzroseBelum ada peringkat
- Case Study 1Dokumen6 halamanCase Study 1rajambal_ayyasamy0% (1)
- Aluminum HydroxideIIDokumen21 halamanAluminum HydroxideIIbayadmomoBelum ada peringkat
- Asthma and COPD NCLEXDokumen17 halamanAsthma and COPD NCLEXPotchiee PfizerBelum ada peringkat
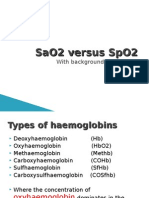
- SaO2 Versus SpO2Dokumen9 halamanSaO2 Versus SpO2jidongjc100% (1)
- Blood Gas Questions With Answers - 1998Dokumen11 halamanBlood Gas Questions With Answers - 1998somarajakBelum ada peringkat
- Guidelines for Measuring Household and Individual Dietary DiversityDari EverandGuidelines for Measuring Household and Individual Dietary DiversityBelum ada peringkat
- Problem-based Approach to Gastroenterology and HepatologyDari EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisBelum ada peringkat
- Normal ValuesDokumen6 halamanNormal Valuesmindreader19Belum ada peringkat
- AbgDokumen7 halamanAbgChin ChanBelum ada peringkat
- Acid Base BalanceDokumen46 halamanAcid Base Balanceleesteph78Belum ada peringkat
- DARDokumen4 halamanDARfritzroseBelum ada peringkat
- B 304Dokumen2 halamanB 304fritzroseBelum ada peringkat
- Maternity NursingDokumen28 halamanMaternity Nursingja100% (11)
- Communicable DiseasesDokumen49 halamanCommunicable Diseasesfritzrose100% (1)
- OR 01b FCDokumen16 halamanOR 01b FCfritzroseBelum ada peringkat
- Acid Base Balance and DisordersDokumen25 halamanAcid Base Balance and DisordersIsmail Vokshi100% (1)
- 2 - Concept Map 4Dokumen4 halaman2 - Concept Map 4keshav singhBelum ada peringkat
- Acid-Base Balance - The Poultry Site PDFDokumen10 halamanAcid-Base Balance - The Poultry Site PDFwl cBelum ada peringkat
- Arterial Blood Gas Interpretation: Associate Professor Dr. Samah ShehataDokumen44 halamanArterial Blood Gas Interpretation: Associate Professor Dr. Samah Shehataraed faisalBelum ada peringkat
- ABG InterpretationDokumen37 halamanABG InterpretationMaliha NaseerBelum ada peringkat
- Acid Base BalanceDokumen44 halamanAcid Base BalanceKenny JapBelum ada peringkat
- VETS - Sheri Ross - Management of Chronic Kidney DiseaseDokumen11 halamanVETS - Sheri Ross - Management of Chronic Kidney DiseaseFerrianto Diyan KusumaBelum ada peringkat
- Exercise 10Dokumen4 halamanExercise 10aker39Belum ada peringkat
- SEP. 2015 RECALLS MRCOG P2 DR HAMADA Aboromuh PDFDokumen95 halamanSEP. 2015 RECALLS MRCOG P2 DR HAMADA Aboromuh PDFuzairBelum ada peringkat
- Reference: Piedad C. Pena (Et Al.) Biochemistry Laboratory Manual - 1 Ed. - Quezon City: C&E Publishing, Inc., 2015Dokumen3 halamanReference: Piedad C. Pena (Et Al.) Biochemistry Laboratory Manual - 1 Ed. - Quezon City: C&E Publishing, Inc., 2015Kris Marie DelaCruz DomingoBelum ada peringkat
- Icu ProtocolDokumen4 halamanIcu Protocolmehal guptaBelum ada peringkat
- Rta and Neurogenic BladderDokumen10 halamanRta and Neurogenic BladdertraceyBelum ada peringkat
- Bicarbonate Therapy in Severe Metabolic AcidosisDokumen39 halamanBicarbonate Therapy in Severe Metabolic AcidosisRoberto UrquizaBelum ada peringkat
- Monitoring and Troubleshooting in Mechanical VentilatorDokumen77 halamanMonitoring and Troubleshooting in Mechanical VentilatorRashma Little RobinBelum ada peringkat
- Clinical Manifestations and Treatment of Hypokalemia in Adults - UpToDateDokumen22 halamanClinical Manifestations and Treatment of Hypokalemia in Adults - UpToDateNguyễn Trịnh Xuân HợpBelum ada peringkat
- OMNI CitrateDokumen2 halamanOMNI CitratePopescu Viorica100% (1)
- General Physiology: APEC Exam Study NotesDokumen9 halamanGeneral Physiology: APEC Exam Study NotesKC PalattaoBelum ada peringkat
- Renal EmergenciesDokumen93 halamanRenal EmergenciesShubham gaurBelum ada peringkat
- CH 67Dokumen40 halamanCH 67Valentina LajqiBelum ada peringkat
- Qdoc - Tips Urology Mcqs For Posgraduate ExamDokumen62 halamanQdoc - Tips Urology Mcqs For Posgraduate ExamDALIABelum ada peringkat
- General Approach To Drug Poisoning in AdultsDokumen14 halamanGeneral Approach To Drug Poisoning in AdultsAnonymous cHPg1bKrotBelum ada peringkat
- Alcoholic KetoacidosisDokumen3 halamanAlcoholic KetoacidosisFaishal HanifBelum ada peringkat
- Acid Base TutorialDokumen74 halamanAcid Base TutorialuedmarineBelum ada peringkat
- Worksheet On Nursing Management of Fluid Electrolyte and Acid Base ImbalancesDokumen3 halamanWorksheet On Nursing Management of Fluid Electrolyte and Acid Base ImbalancesMa. Ferimi Gleam BajadoBelum ada peringkat
- Drug Study MixDokumen29 halamanDrug Study MixMatty JolbitadoBelum ada peringkat
- Patho Metabolic AcidosisDokumen5 halamanPatho Metabolic Acidosisapi-285177380Belum ada peringkat
- Overview of The Management of Acute Kidney Injury in Adults - UpToDateDokumen13 halamanOverview of The Management of Acute Kidney Injury in Adults - UpToDateDaniely FreitasBelum ada peringkat
- PHARCHEM1 Lec C3Dokumen6 halamanPHARCHEM1 Lec C3qwertyuioppoiuewqBelum ada peringkat