Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- QD 002 - Quality Manual 2022 - Feb22-Rev2.6 - RBDokumen35 halamanQD 002 - Quality Manual 2022 - Feb22-Rev2.6 - RBAjibade SukuratBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Rheumatoid Arthritis Skin ManifestationsDokumen2 halamanRheumatoid Arthritis Skin ManifestationsRiena Austine Leonor NarcillaBelum ada peringkat
- A Christian Perspective of Acupuncture: A Research Paper Submitted To DR Keith WarringtonDokumen33 halamanA Christian Perspective of Acupuncture: A Research Paper Submitted To DR Keith WarringtonEric TBelum ada peringkat
- 5 - DystociaDokumen43 halaman5 - DystociaMara Medina - BorleoBelum ada peringkat
- Obstruksi Usus (Bowel Obstruction)Dokumen7 halamanObstruksi Usus (Bowel Obstruction)bhatubimBelum ada peringkat
- Obstruksi Usus (Bowel Obstruction)Dokumen7 halamanObstruksi Usus (Bowel Obstruction)bhatubimBelum ada peringkat
- Miethke DualSwitch Valve in Lumboperitoneal ShuntsDokumen9 halamanMiethke DualSwitch Valve in Lumboperitoneal ShuntsRosa SelviaBelum ada peringkat
- Changes in The Volumes of The Brain and Cerebrospinal Fluid Spaces After ShuntDokumen6 halamanChanges in The Volumes of The Brain and Cerebrospinal Fluid Spaces After ShuntRosa SelviaBelum ada peringkat
- HHD LVHDokumen10 halamanHHD LVHRosa SelviaBelum ada peringkat
- Changes in The Volumes of The Brain and Cerebrospinal Fluid Spaces After ShuntDokumen6 halamanChanges in The Volumes of The Brain and Cerebrospinal Fluid Spaces After ShuntRosa SelviaBelum ada peringkat
- Headaches in Patients With Shunts RekateDokumen4 halamanHeadaches in Patients With Shunts RekateRosa SelviaBelum ada peringkat
- ContentDokumen8 halamanContentRosa SelviaBelum ada peringkat
- Stroke Model of CareDokumen83 halamanStroke Model of CareRosa SelviaBelum ada peringkat
- Acute Stroke GuidelineDokumen36 halamanAcute Stroke GuidelineRosa SelviaBelum ada peringkat
- Office Management & Administration Skills Training Course - GLOMACSDokumen4 halamanOffice Management & Administration Skills Training Course - GLOMACSKyaw Min HanBelum ada peringkat
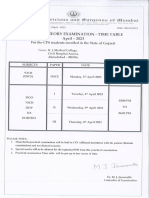
- DCH Time TableDokumen1 halamanDCH Time TableGane HospitalBelum ada peringkat
- Webinar - I-WPS OfficeDokumen31 halamanWebinar - I-WPS OfficeGayathri sundarajanBelum ada peringkat
- Albatex® CoDokumen16 halamanAlbatex® CoMahbubul HasanBelum ada peringkat
- Highcontainment BiolabsDokumen84 halamanHighcontainment Biolabshansley cookBelum ada peringkat
- الاشتريه في الوزاريات 6 اعدادي اشتر احمد 2023 كونيكاDokumen132 halamanالاشتريه في الوزاريات 6 اعدادي اشتر احمد 2023 كونيكاSajad HussienBelum ada peringkat
- Brokenshire College Socsksargen, Inc.: NCM 100-Theorerical Foundations in NursingDokumen8 halamanBrokenshire College Socsksargen, Inc.: NCM 100-Theorerical Foundations in NursingKeren Happuch EspirituBelum ada peringkat
- Skoll World Forum Panel - FINALDokumen16 halamanSkoll World Forum Panel - FINALNara E AíBelum ada peringkat
- Job Satisfaction ProjectDokumen8 halamanJob Satisfaction ProjectSwetha Reddy Lingala100% (2)
- 19th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation AssociationDokumen3 halaman19th Annual Scientific Meeting of Indonesian Physical Medicine and Rehabilitation AssociationNia Kania HapsyahBelum ada peringkat
- Readiness, Barriers and Potential Strenght of Nursing in Implementing Evidence-Based PracticeDokumen9 halamanReadiness, Barriers and Potential Strenght of Nursing in Implementing Evidence-Based PracticeWahyu HidayatBelum ada peringkat
- Tbf-531Bodyfat Monitor/Scale: Instruction ManualDokumen13 halamanTbf-531Bodyfat Monitor/Scale: Instruction ManualJose JimenoBelum ada peringkat
- Better BalanceDokumen13 halamanBetter BalanceMiriam NovoBelum ada peringkat
- Orthogold100 Ow100usDokumen70 halamanOrthogold100 Ow100uslumitransBelum ada peringkat
- Reflection Paper1 Psy111-1 A41Dokumen1 halamanReflection Paper1 Psy111-1 A41owyyyBelum ada peringkat
- Theme 4 - Fixation and Stabilization of PRADDokumen3 halamanTheme 4 - Fixation and Stabilization of PRADShany SchwarzwaldBelum ada peringkat
- 32 SMS - Cleaning Vessel (Air Line)Dokumen6 halaman32 SMS - Cleaning Vessel (Air Line)Mohd KhaidirBelum ada peringkat
- The Hahnemannian Monthly1879pdfDokumen831 halamanThe Hahnemannian Monthly1879pdfBruntBelum ada peringkat
- Eyes RETDEMDokumen2 halamanEyes RETDEMRenz Kier L. ComaBelum ada peringkat
- Pharma - M6L2 - Drug Therapy For OA and Gouty ArthritisDokumen8 halamanPharma - M6L2 - Drug Therapy For OA and Gouty ArthritisAngelaTrinidadBelum ada peringkat
- Calculating Pediatric Medication and Fluid DosagesDokumen5 halamanCalculating Pediatric Medication and Fluid DosagesMayank KumarBelum ada peringkat
- 02 - February RsmiDokumen123 halaman02 - February RsmiAlex SibalBelum ada peringkat
- Sitting Kills, Moving Heals. An Interview With Dr. Joan VernikosDokumen25 halamanSitting Kills, Moving Heals. An Interview With Dr. Joan Vernikosjayjonbeach100% (1)
- Test BFQDokumen13 halamanTest BFQChristian100% (3)
- BCM School BasantAv enueDugr iLudhi ana Cl ass-V. Subj ect-Sci ence Apti tudeWor ksheet and Honey beesDokumen6 halamanBCM School BasantAv enueDugr iLudhi ana Cl ass-V. Subj ect-Sci ence Apti tudeWor ksheet and Honey beesParam stationersBelum ada peringkat
- Sample Writing Practice Test 2Dokumen6 halamanSample Writing Practice Test 2Hồ TrânBelum ada peringkat