Anda mungkin juga menyukai
- Polycystic Ovary Syndrome: Understanding Ovaries and OvulationDokumen5 halamanPolycystic Ovary Syndrome: Understanding Ovaries and OvulationBhavik ShahBelum ada peringkat
- Power Over Pcos EbookDokumen160 halamanPower Over Pcos EbookIra Ayu Lestari100% (2)
- Acupuncture Endometriosis and Chinese MedicineDokumen7 halamanAcupuncture Endometriosis and Chinese MedicineRezqi N FirdaBelum ada peringkat
- Thyroid Symptom HackerDokumen18 halamanThyroid Symptom HackerozergyalmoBelum ada peringkat
- Microbiome impact on sex, thyroid, growth and parathyroid hormonesDokumen13 halamanMicrobiome impact on sex, thyroid, growth and parathyroid hormonesBrenda FolkBelum ada peringkat
- Top 8 Hormones You Need to Know AboutDokumen15 halamanTop 8 Hormones You Need to Know AboutBarbara100% (1)
- 12 Health & Fitness Mistakes You Don'T Know You'Re Making: Michael MatthewsDokumen61 halaman12 Health & Fitness Mistakes You Don'T Know You'Re Making: Michael MatthewsJovan Steam100% (1)
- Parathyroid GlandsDokumen4 halamanParathyroid GlandsMary Grace Buscargas PolancosBelum ada peringkat
- Diet InfoDokumen19 halamanDiet Infoathena19Belum ada peringkat
- Hormone Guide CCDokumen11 halamanHormone Guide CCbroBelum ada peringkat
- GutRepair Top25 HerbsDokumen29 halamanGutRepair Top25 HerbsOlli PostiBelum ada peringkat
- Bioidentical Hormones-2-1Dokumen2 halamanBioidentical Hormones-2-1api-206847705Belum ada peringkat
- Dysbiosis QuestionnaireDokumen2 halamanDysbiosis QuestionnairekenetmartinBelum ada peringkat
- PCOS and Infertility - Causes and TreatmentDokumen42 halamanPCOS and Infertility - Causes and TreatmentlouloucheBelum ada peringkat
- Nutrition and Diet Therapy for AdulthoodDokumen26 halamanNutrition and Diet Therapy for AdulthoodDominic AlmendrasBelum ada peringkat
- Kalonji Benefits ImpDokumen18 halamanKalonji Benefits Impjas899100% (1)
- Diet Plan of Different DiseasesDokumen43 halamanDiet Plan of Different DiseasesSanaBelum ada peringkat
- Copper DeficiencyDokumen30 halamanCopper DeficiencyMathewos MekonnenBelum ada peringkat
- Healthy, Happy Gut Summit™: Everything You Need To Know About Probiotics Michael RuscioDokumen15 halamanHealthy, Happy Gut Summit™: Everything You Need To Know About Probiotics Michael RuscioMiha VucBelum ada peringkat
- Synergy Science: The Benefits of Echo WaterDokumen9 halamanSynergy Science: The Benefits of Echo WaterSubbaraju GvBelum ada peringkat
- What is DetoxificationDokumen6 halamanWhat is DetoxificationLaila AbdulBelum ada peringkat
- 20 Pain Cures in Our Kitchen CupboardDokumen24 halaman20 Pain Cures in Our Kitchen CupboardNISAR_786Belum ada peringkat
- Disorders of The ColonDokumen47 halamanDisorders of The ColonGieve BlasurcaBelum ada peringkat
- Hormone Health: How to Get Your Hormones Back in BalanceDokumen9 halamanHormone Health: How to Get Your Hormones Back in BalanceHarindra DunuwilaBelum ada peringkat
- Estrogen DominanceDokumen39 halamanEstrogen DominanceJen AlkinsBelum ada peringkat
- Oxalate Control: The Great Plains Laboratory, IncDokumen4 halamanOxalate Control: The Great Plains Laboratory, IncMaria Plaias100% (1)
- Insulin Resistance & Green TeaDokumen6 halamanInsulin Resistance & Green TeaSrinivasan GanapathiBelum ada peringkat
- The Steroidogenic PathwayDokumen47 halamanThe Steroidogenic Pathwaysusan64Belum ada peringkat
- Colostrum PDFDokumen43 halamanColostrum PDFypatia41100% (1)
- Role of Magnesium and CalciumDokumen5 halamanRole of Magnesium and CalciumsemiBelum ada peringkat
- Vitamins and MineralsDokumen8 halamanVitamins and MineralsDikshaBelum ada peringkat
- DR Cabral 7 Day Functional Liver Detox Protocol PDFDokumen20 halamanDR Cabral 7 Day Functional Liver Detox Protocol PDFTyler RelphBelum ada peringkat
- Astragalus Root Can Prevent Telomere ShorteningDokumen10 halamanAstragalus Root Can Prevent Telomere Shorteningklumsy15Belum ada peringkat
- Blood Test Interpretation PDFDokumen10 halamanBlood Test Interpretation PDFstore.hrBelum ada peringkat
- Foods To AvoidDokumen3 halamanFoods To AvoidInqueBelum ada peringkat
- Immune System FormulasDokumen3 halamanImmune System FormulasKasiaBelum ada peringkat
- Bicarbonate Spdium-2260 Paper - FullDokumen10 halamanBicarbonate Spdium-2260 Paper - FullDel Valle MauroBelum ada peringkat
- 3 Transcripts From The Adrenal Solutions SummitDokumen39 halaman3 Transcripts From The Adrenal Solutions SummitPatriciaPedroGomesBelum ada peringkat
- Medical Medium Thyroid Healing TestimonialsDokumen15 halamanMedical Medium Thyroid Healing TestimonialsGeri SulanjakuBelum ada peringkat
- Preparing For Your Detox The Pre Tox ProtocolDokumen28 halamanPreparing For Your Detox The Pre Tox ProtocolcarlosBelum ada peringkat
- Vitamin E ReportDokumen10 halamanVitamin E ReportGia DelpanBelum ada peringkat
- Protein EssentialsDokumen49 halamanProtein Essentialsarun100% (2)
- Improve Stomach Acid in 1 Minute with This Simple DrinkDokumen5 halamanImprove Stomach Acid in 1 Minute with This Simple DrinkAysen Kahyaoglu TaylorBelum ada peringkat
- Health Psychology Assignment (MA201477)Dokumen7 halamanHealth Psychology Assignment (MA201477)Syeda DaniaBelum ada peringkat
- CandidaDokumen1 halamanCandidalopansBelum ada peringkat
- My Wobenzym Testimony - by Dr. Joseph J. CollinsDokumen2 halamanMy Wobenzym Testimony - by Dr. Joseph J. Collinstimsmith1081574Belum ada peringkat
- The Bone Broth Diet PlusDokumen21 halamanThe Bone Broth Diet Pluspeter abilezBelum ada peringkat
- Handout Elimination Diet PatientDokumen6 halamanHandout Elimination Diet PatientKateOpulenciaBelum ada peringkat
- Factsheet Food Sources of Soluble FibreDokumen4 halamanFactsheet Food Sources of Soluble FibreanandkishoreBelum ada peringkat
- Leptin Hormone Dramatically Spur Weight LossDokumen3 halamanLeptin Hormone Dramatically Spur Weight LossredeveilBelum ada peringkat
- BIG Masterclass Mastery Session 1 TranscriptDokumen9 halamanBIG Masterclass Mastery Session 1 TranscriptbabalaboxBelum ada peringkat
- Wahlsdietcheatsheet Level 1Dokumen1 halamanWahlsdietcheatsheet Level 1janeBelum ada peringkat
- Metabolic Typing TestDokumen16 halamanMetabolic Typing TestKendall Rusco100% (1)
- Animal Protein Vs Plant Protein.Dokumen7 halamanAnimal Protein Vs Plant Protein.Emmanuel Charles100% (1)
- The Most Important Medical TestDokumen5 halamanThe Most Important Medical Testsrinivasan9Belum ada peringkat
- Boost Your Thinking, Memory, Mood and Focus: in MinutesDokumen24 halamanBoost Your Thinking, Memory, Mood and Focus: in MinutesGagandeep Singh karir100% (1)
- Constipation Care in Cancer PatientsDokumen2 halamanConstipation Care in Cancer PatientsFayruz Zahrotin NiswahBelum ada peringkat
- Headache QuestionnaireDokumen10 halamanHeadache QuestionnairePerisha VeeraBelum ada peringkat
- Carb Cycling for Weight Loss: A Beginner’s 3-Week Guide with Sample Curated RecipesDari EverandCarb Cycling for Weight Loss: A Beginner’s 3-Week Guide with Sample Curated RecipesBelum ada peringkat
- Abortion and Post Traumatic Stress Disorder - TheresaDokumen5 halamanAbortion and Post Traumatic Stress Disorder - TheresaPooja AcharyaBelum ada peringkat
- Trismus Aetiology Differentialdiagnosisandtreatment99616Dokumen5 halamanTrismus Aetiology Differentialdiagnosisandtreatment99616Ellizabeth LilantiBelum ada peringkat
- Is a Tooth with a Root Canal Perforation DoomedDokumen2 halamanIs a Tooth with a Root Canal Perforation DoomedPooja AcharyaBelum ada peringkat
- Trismus Aetiology Differentialdiagnosisandtreatment99616Dokumen5 halamanTrismus Aetiology Differentialdiagnosisandtreatment99616Ellizabeth LilantiBelum ada peringkat
- Clin Pharmacy ADRDokumen36 halamanClin Pharmacy ADRAnonymous DgPsK0oQBelum ada peringkat
- Cardiovascular Test Questions: "I Will Observe The Color of My Urine and Stool"Dokumen36 halamanCardiovascular Test Questions: "I Will Observe The Color of My Urine and Stool"Melodia Turqueza GandezaBelum ada peringkat
- DRUG STUDY SpironolactoneDokumen4 halamanDRUG STUDY SpironolactoneJerremy LuqueBelum ada peringkat
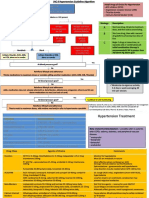
- JNC 8 Hypertension Guideline AlgorithmDokumen2 halamanJNC 8 Hypertension Guideline Algorithmnaila inayatiBelum ada peringkat
- 2006, Vol.24, Issues 2, Women's DermatologyDokumen145 halaman2006, Vol.24, Issues 2, Women's DermatologyRizweta DestinBelum ada peringkat
- OILY SKIN A Review of Treatment Options PDFDokumen7 halamanOILY SKIN A Review of Treatment Options PDFgirvBelum ada peringkat
- Modern Management of AcneDokumen5 halamanModern Management of Acnediana romeroBelum ada peringkat
- Mr. William's Case StudyDokumen2 halamanMr. William's Case StudyChelsea AquinoBelum ada peringkat
- Diuretic DrugsDokumen62 halamanDiuretic DrugsAbdul WahabBelum ada peringkat
- Lifestyle Changes and Medications for Treating Polycystic Ovarian SyndromeDokumen13 halamanLifestyle Changes and Medications for Treating Polycystic Ovarian SyndromeAnonymous PuaFsusBelum ada peringkat
- Summer Training Guide For Pharmacy Students-1Dokumen132 halamanSummer Training Guide For Pharmacy Students-1Rania T. Sabri100% (2)
- OPD MedicineDokumen10 halamanOPD Medicinehusnain nadeemBelum ada peringkat
- Treatment Ciroza HepaticaDokumen85 halamanTreatment Ciroza HepaticaMarina TrofimciucBelum ada peringkat
- I CARE Early COVID ProtocolDokumen36 halamanI CARE Early COVID ProtocolOana BarburaBelum ada peringkat
- Transsexual Transgendered Guide To Obtaining and Using Transsexual Hormones, Hormone Replacement Therapy HRTDokumen52 halamanTranssexual Transgendered Guide To Obtaining and Using Transsexual Hormones, Hormone Replacement Therapy HRTTrinity Rose Transsexual77% (13)
- I CARE Early COVID Protocol 2023 03 30Dokumen34 halamanI CARE Early COVID Protocol 2023 03 30BugMagnetBelum ada peringkat
- 2008 AnnualDokumen100 halaman2008 AnnualKori PratiwiBelum ada peringkat
- Treatment of Liver CirrhosisDokumen85 halamanTreatment of Liver CirrhosisPetru Boaghi100% (1)
- Board Exam Mock QuestionsDokumen34 halamanBoard Exam Mock QuestionsglenBelum ada peringkat
- Perindopril ErbumineDokumen8 halamanPerindopril ErbumineYanna Habib-MangotaraBelum ada peringkat
- Sind Ovario Poliquistico 2016 - NejmDokumen11 halamanSind Ovario Poliquistico 2016 - NejmAntonio MoncadaBelum ada peringkat
- Internal Medicine Mar 2022Dokumen8 halamanInternal Medicine Mar 2022Sanielle Karla Garcia LorenzoBelum ada peringkat
- Andrology - 2017 - Semet - The Impact of Drugs On Male Fertility A ReviewDokumen24 halamanAndrology - 2017 - Semet - The Impact of Drugs On Male Fertility A ReviewAbhishek RampalBelum ada peringkat
- HS treatment options under 40 charactersDokumen52 halamanHS treatment options under 40 charactersRenzo Cruz CaldasBelum ada peringkat
- Nursing Care for Liver Cirrhosis Patient on SpironolactoneDokumen2 halamanNursing Care for Liver Cirrhosis Patient on SpironolactoneNathalia CabalseBelum ada peringkat
- West Visayas State University Drug StudyDokumen4 halamanWest Visayas State University Drug StudyLene ThereseBelum ada peringkat
- 50 Item Pharmacology Exam With Answers and RationaleDokumen17 halaman50 Item Pharmacology Exam With Answers and Rationalebibot189% (18)
- Common Toxicology Calls GuideDokumen4 halamanCommon Toxicology Calls GuideDimitriy SmolyanskiyBelum ada peringkat
- HRT Protocols Integrative WellnessDokumen8 halamanHRT Protocols Integrative WellnessGutoGonçalves100% (1)
- Nursing Pharmacology Sample Exam QuestionsDokumen3 halamanNursing Pharmacology Sample Exam QuestionsDhreambhig Ahrchorphul100% (1)