Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Mitral RegurgitationDokumen6 halamanMitral RegurgitationMelfi Triani SiskaBelum ada peringkat
- Casereport-Modified Radical MastectomyDokumen33 halamanCasereport-Modified Radical MastectomyMayflor de LunaBelum ada peringkat
- Ultrasound Evaluation of Abnormal Ovarian Cysts and Solid MassesDokumen43 halamanUltrasound Evaluation of Abnormal Ovarian Cysts and Solid MassesibmreadywriterBelum ada peringkat
- CT Brain Perfusion in The Acute Stroke Setting Maria ScottiDokumen52 halamanCT Brain Perfusion in The Acute Stroke Setting Maria ScottiDedi Sutia100% (1)
- MRCPCH - Important Skin DiseasesDokumen42 halamanMRCPCH - Important Skin DiseasesarjumandBelum ada peringkat
- Dr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaDokumen10 halamanDr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaOnkologi Radiasi Angkatan 23Belum ada peringkat
- The Epic of GilgameshDokumen4 halamanThe Epic of GilgameshChristelle GarciaBelum ada peringkat
- Confounding in EpidemiologyDokumen36 halamanConfounding in Epidemiologynivasa reddy100% (1)
- Legal Issues Affecting MHN 2Dokumen15 halamanLegal Issues Affecting MHN 2Christelle GarciaBelum ada peringkat
- Management of Stage III Non-Small Cell Lung Cancer - UpToDateDokumen23 halamanManagement of Stage III Non-Small Cell Lung Cancer - UpToDateRasheid MekkiBelum ada peringkat
- Chapter - 004 Health AssessmentDokumen10 halamanChapter - 004 Health AssessmentTrixie AlvarezBelum ada peringkat
- Neuroimaging Clinics of North America 2015 #2 PDFDokumen173 halamanNeuroimaging Clinics of North America 2015 #2 PDFYully gunawan100% (1)
- Garcia, Christelle Guiang, Abegail Jerez, Rizzia Oppositional Defiant BehaviorDokumen4 halamanGarcia, Christelle Guiang, Abegail Jerez, Rizzia Oppositional Defiant BehaviorChristelle GarciaBelum ada peringkat
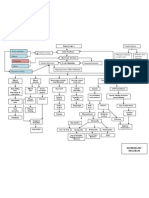
- Diabetes Mellitus Type 2 Schematic DiagramDokumen1 halamanDiabetes Mellitus Type 2 Schematic DiagramChristelle GarciaBelum ada peringkat
- Patterns For PPRDokumen5 halamanPatterns For PPRChristelle GarciaBelum ada peringkat
- Radiologi ILO Terbaru (PIPKRA 2011)Dokumen47 halamanRadiologi ILO Terbaru (PIPKRA 2011)elsaBelum ada peringkat
- Definition of PhimosisDokumen11 halamanDefinition of PhimosisAzizah Hafaz0% (1)
- Management of Irritational Fibroma by Three Different Treatment Modalities - A Case SeriesDokumen4 halamanManagement of Irritational Fibroma by Three Different Treatment Modalities - A Case SeriesInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Hansen1985 Proliferative Verrucous LeukoplakiaDokumen14 halamanHansen1985 Proliferative Verrucous LeukoplakiaJulia FerigattoBelum ada peringkat
- Cervical Cancer Screening - DOH Standard - May 2018Dokumen14 halamanCervical Cancer Screening - DOH Standard - May 2018Basil al-hashaikehBelum ada peringkat
- Hypothalamus-Pituitary-Thyroid Axis: PRESENTERS: DR: Nyangaresi Justine DR: Mitchelle Facilitator: DRDokumen31 halamanHypothalamus-Pituitary-Thyroid Axis: PRESENTERS: DR: Nyangaresi Justine DR: Mitchelle Facilitator: DRJustine NyangaresiBelum ada peringkat
- PansitopeniaDokumen33 halamanPansitopeniaBrad WrightBelum ada peringkat
- Safety Data Sheet: 1. IdentificationDokumen8 halamanSafety Data Sheet: 1. IdentificationShinthya DewiBelum ada peringkat
- Update NCCN 2018Dokumen11 halamanUpdate NCCN 2018Deddy Setiawan WidjajaBelum ada peringkat
- The Efficacy and Safety of Sunscreen Use For The Prevention of Skin CancerDokumen7 halamanThe Efficacy and Safety of Sunscreen Use For The Prevention of Skin CancerBryan NguyenBelum ada peringkat
- Developmental Anamolies of Soft Tissues of Oral CavityDokumen73 halamanDevelopmental Anamolies of Soft Tissues of Oral Cavityvellingiriramesh53040% (1)
- Insights ImmunotherapyDokumen32 halamanInsights Immunotherapy@yuanBelum ada peringkat
- Kumar DeepDokumen12 halamanKumar Deepkumardeep DuttaBelum ada peringkat
- Rectal AdenocarcinomaDokumen93 halamanRectal AdenocarcinomaLara MenBelum ada peringkat
- Prophylactic MastectomyDokumen5 halamanProphylactic MastectomyMuhammad Darussalam DarwisBelum ada peringkat
- Hematuria: Gross Versus Microscopic HematuriaDokumen2 halamanHematuria: Gross Versus Microscopic HematuriaShintia Theresia LumempouwBelum ada peringkat
- Buccal Mucosa CancerDokumen9 halamanBuccal Mucosa Cancermuhammad_ariefBelum ada peringkat
- PHD ProposalDokumen21 halamanPHD ProposalHAIMANOTBelum ada peringkat
- Head and Neck Laryngeal Tumors An OverviewDokumen7 halamanHead and Neck Laryngeal Tumors An OverviewpupuayuwandiraBelum ada peringkat
- Informative Speech 1Dokumen3 halamanInformative Speech 1Janiela MarieBelum ada peringkat