Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Hypertension - A Companion To Braunwald - S Heart Disease 3rd Edition (2017)Dokumen503 halamanHypertension - A Companion To Braunwald - S Heart Disease 3rd Edition (2017)JOLANDA ANGELIN100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Cva CPDokumen53 halamanCva CPApol Pen100% (2)
- Nursing Management of HypertensionDokumen152 halamanNursing Management of HypertensionEnfermeriaAncam100% (3)
- Comprehensive Nclex Notes - Easy To ReadDokumen97 halamanComprehensive Nclex Notes - Easy To ReadBilal Yousuf98% (58)
- Ati QuestionsDokumen2 halamanAti Questionsnjames44Belum ada peringkat
- Neuro QuizDokumen47 halamanNeuro QuizMeredith Caitlyn Fernandez100% (1)
- Antenatal CareDokumen19 halamanAntenatal CareIshika RoyBelum ada peringkat
- Hijama PointsDokumen23 halamanHijama PointsShahbaz Ahmed100% (1)
- RH Incompatibility HandoutDokumen4 halamanRH Incompatibility HandoutMaricar Sanson FelicianoBelum ada peringkat
- Pediatric Nursing, Introduction To Maternity and Pediatric NursingDokumen82 halamanPediatric Nursing, Introduction To Maternity and Pediatric NursingJose Joseph0% (1)
- Clerkship Handbook: Family MedicineDokumen51 halamanClerkship Handbook: Family MedicineKen WonBelum ada peringkat
- Role of Nurse-Non Communicable DiseasesDokumen105 halamanRole of Nurse-Non Communicable DiseasesKrishnaveni MurugeshBelum ada peringkat
- Config Measure Tab Aortic Folder LVOT Trace Folder Make Sure LVOT VTI Is TickedDokumen1 halamanConfig Measure Tab Aortic Folder LVOT Trace Folder Make Sure LVOT VTI Is TickedOnon EssayedBelum ada peringkat
- CRT in Narrow QRSDokumen11 halamanCRT in Narrow QRSOnon EssayedBelum ada peringkat
- The End of Metabolic SyndromeDokumen6 halamanThe End of Metabolic SyndromeOnon EssayedBelum ada peringkat
- Life Style ModificationDokumen11 halamanLife Style ModificationOnon Essayed100% (1)
- Rethinking Hypertension in The 21st Century: An Overview of The Expanded Definition and Classification of Hypertension CMEDokumen19 halamanRethinking Hypertension in The 21st Century: An Overview of The Expanded Definition and Classification of Hypertension CMEOnon EssayedBelum ada peringkat
- SITAGLIPTINDokumen15 halamanSITAGLIPTINOnon EssayedBelum ada peringkat
- Embedded Systems: Calibration Instruments LaboratoryDokumen12 halamanEmbedded Systems: Calibration Instruments LaboratoryAlsacia PixBelum ada peringkat
- Elective II Group 1 Chronic IllnessDokumen31 halamanElective II Group 1 Chronic IllnessAldrine Albor Anyayahan IBelum ada peringkat
- Celery Seed PDFDokumen2 halamanCelery Seed PDFElviiSuhainiiSr.Belum ada peringkat
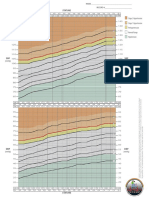
- BP Chart Girls Color WideDokumen1 halamanBP Chart Girls Color WidealbertBelum ada peringkat
- Journal Coartation AortaDokumen6 halamanJournal Coartation AortaMangaismeBelum ada peringkat
- Teachers Health Examination FormDokumen2 halamanTeachers Health Examination FormRosemarie Ceredon ChyBelum ada peringkat
- Tingkat Kepatuhan Antihipertensi Dan Pengontrolan Tekanan Darah Pasien Rawat Jalan Rs Pku Muhammadiyah BantulDokumen6 halamanTingkat Kepatuhan Antihipertensi Dan Pengontrolan Tekanan Darah Pasien Rawat Jalan Rs Pku Muhammadiyah BantulRusnaneeBelum ada peringkat
- Hypertension Clinical Study PDFDokumen42 halamanHypertension Clinical Study PDFsertti23Belum ada peringkat
- Presented By: Jagdish Sambad M.SC - Nursing, Ikdrc College of NursingDokumen80 halamanPresented By: Jagdish Sambad M.SC - Nursing, Ikdrc College of NursingAdia MasooraBelum ada peringkat
- Health Salt 2Dokumen7 halamanHealth Salt 2Nithyalawrence LawrenceBelum ada peringkat
- Health Appraisal Record AY 2020Dokumen1 halamanHealth Appraisal Record AY 2020jinBelum ada peringkat
- Predicting and Detection of Heart Disease Using Machine LearningDokumen19 halamanPredicting and Detection of Heart Disease Using Machine Learningstudent lifeBelum ada peringkat
- Blood Pressure ProjectDokumen3 halamanBlood Pressure ProjectjademvdfBelum ada peringkat
- Decreased Cardiac Output Related To Decreased Venous Return: Level of PrioritizationDokumen3 halamanDecreased Cardiac Output Related To Decreased Venous Return: Level of PrioritizationKryza Dale Bunado BaticanBelum ada peringkat
- Plan of Care PaperDokumen5 halamanPlan of Care Paperapi-548969267Belum ada peringkat
- A Study To Assess The Effectiveness of Abdominal Breathing Exercise in Reduction of Blood Pressure Among Hypertensive Patients in Selected Hospitals at BhopalDokumen6 halamanA Study To Assess The Effectiveness of Abdominal Breathing Exercise in Reduction of Blood Pressure Among Hypertensive Patients in Selected Hospitals at BhopalEditor IJTSRDBelum ada peringkat
- MedicineDokumen48 halamanMedicineKasun Perera0% (1)
- Cardiovascular NCLEX QuestionsDokumen12 halamanCardiovascular NCLEX QuestionsAivan Karl AmbaganBelum ada peringkat