Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- 5 RW DW LRQ) O DSV: NjurxqgDokumen3 halaman5 RW DW LRQ) O DSV: Njurxqgpredrag_maksimovichBelum ada peringkat
- Head and Neck Cancer - Resection and Neck DissectionDokumen4 halamanHead and Neck Cancer - Resection and Neck Dissectionpredrag_maksimovichBelum ada peringkat
- Hearing Impairment: Print TopicDokumen2 halamanHearing Impairment: Print Topicpredrag_maksimovichBelum ada peringkat
- Bells Palsy and Mona LisaDokumen3 halamanBells Palsy and Mona Lisapredrag_maksimovichBelum ada peringkat
- Ent Recommended Reading ListDokumen1 halamanEnt Recommended Reading Listpredrag_maksimovichBelum ada peringkat
- Ultimate Field Guide To PhotographyDokumen23 halamanUltimate Field Guide To PhotographyIulian Oprea100% (1)
- ABC of AIDSDokumen126 halamanABC of AIDSmufaddal83Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
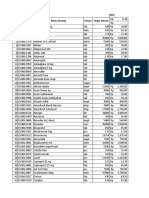
- Harga ObatDokumen44 halamanHarga ObatFreddy ApotekerBelum ada peringkat
- CotrimoxazoleDokumen3 halamanCotrimoxazolecsy123Belum ada peringkat
- Hubungan Pengetahuan, Sikap dan Tindakan Keluarga dengan Pencegahan TB Paru AktifDokumen124 halamanHubungan Pengetahuan, Sikap dan Tindakan Keluarga dengan Pencegahan TB Paru AktifWilma arifinBelum ada peringkat
- Cology Final McqsDokumen33 halamanCology Final McqsSameer AliBelum ada peringkat
- Super Salida Especial-Mes de Junio ActualizadaDokumen90 halamanSuper Salida Especial-Mes de Junio ActualizadaDiego PazmiñoBelum ada peringkat
- RASPRODokumen36 halamanRASPROVera Yulianti100% (2)
- CroupDokumen20 halamanCroupFariezuan HamidBelum ada peringkat
- The Effects of Laparoscopic Nissen FundoplicationDokumen2 halamanThe Effects of Laparoscopic Nissen FundoplicationGabriel CassBelum ada peringkat
- CSU College of Medicine Obstetrics and Gynecology Department DocumentDokumen10 halamanCSU College of Medicine Obstetrics and Gynecology Department DocumentArianne Joy C. TamarayBelum ada peringkat
- CMA - Culture - First Aid BMP - MCHDokumen8 halamanCMA - Culture - First Aid BMP - MCHSauharda DhakalBelum ada peringkat
- 100 MCQsDokumen35 halaman100 MCQsBader AlMajedBelum ada peringkat
- Antifungal PDFDokumen3 halamanAntifungal PDFFaten SarhanBelum ada peringkat
- Approach To Febrile PatientDokumen79 halamanApproach To Febrile Patientadaneyihune100% (5)
- Medication ListDokumen14 halamanMedication ListMarie LeyvaBelum ada peringkat
- Urtikaria Kronik IdiopatikDokumen6 halamanUrtikaria Kronik IdiopatikgendisBelum ada peringkat
- Puskesmas Sungai Kalu Requests Additional Medical SuppliesDokumen5 halamanPuskesmas Sungai Kalu Requests Additional Medical Suppliesyona firdali rantiBelum ada peringkat
- History of Present Illness: Sample of History Taking Chief Complaint: Chest PainDokumen2 halamanHistory of Present Illness: Sample of History Taking Chief Complaint: Chest PainNeil AlviarBelum ada peringkat
- Dexamethasone (RX) : Dosing & UsesDokumen4 halamanDexamethasone (RX) : Dosing & UsesFauzi GanihBelum ada peringkat
- 兒科Dokumen10 halaman兒科Chia Hsun LinBelum ada peringkat
- What Are The Symptoms Measles (Focus On Measles More, Then Talk About Mumps and Rubella)Dokumen2 halamanWhat Are The Symptoms Measles (Focus On Measles More, Then Talk About Mumps and Rubella)RexDavidGidoBelum ada peringkat
- AzithromycinDokumen1 halamanAzithromycinjennelyn losantaBelum ada peringkat
- Revised Drug IndexDokumen76 halamanRevised Drug IndexMinette SantosBelum ada peringkat
- Medical Declaration Form SummaryDokumen1 halamanMedical Declaration Form SummaryRamBelum ada peringkat
- Drug Study..Dokumen4 halamanDrug Study..Micah SalesBelum ada peringkat
- Prenatal Care Questions and AnswersDokumen6 halamanPrenatal Care Questions and Answersdhodejun lizhaldeBelum ada peringkat
- Metformin in PCOSDokumen5 halamanMetformin in PCOSbalaramBelum ada peringkat
- ASAM AMOXICILLIN MEFENAMAT ANTASIDA ACETYLCYSTEINE AMBROXOLDokumen6 halamanASAM AMOXICILLIN MEFENAMAT ANTASIDA ACETYLCYSTEINE AMBROXOLAgil tri puji lestariBelum ada peringkat
- 100Dokumen15 halaman100Samar FakhryBelum ada peringkat
- Dispensing DrugsDokumen1 halamanDispensing DrugsIan CalalangBelum ada peringkat
- Dosage and effects of ampicillinDokumen1 halamanDosage and effects of ampicillinkimglaidyl bontuyanBelum ada peringkat