Faecal Incontinence in Adults - Review
Diunggah oleh
i can always make u smile :DDeskripsi Asli:
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Faecal Incontinence in Adults - Review
Diunggah oleh
i can always make u smile :DHak Cipta:
Format Tersedia
Review
Faecal incontinence in adults
Robert D Madoff, Susan C Parker, Madhulika G Varma, Ann C Lowry Lancet 2004; 364: 621–32
Division of Colon and Rectal
Faecal incontinence can affect individuals of all ages and in many cases greatly impairs quality of life, but Surgery, Department of
Surgery, University of
incontinent patients should not accept their debility as either inevitable or untreatable. Education of the general
Minnesota, Minneapolis, MN,
public and of health-care providers alike is important, because most cases are readily treatable. Many cases of mild USA (R D Madoff MD,
incontinence respond to simple medical therapy, whereas patients with more advanced incontinence are best cared S C Parker MD, A C Lowry MD)
for after complete physiological assessment. Recent advances in therapy have led to promising results, even for and Department of Surgery,
University of California, San
patients with refractory incontinence. Health-care providers must make every effort to communicate fully with
Francisco, CA (M G Varma MD)
incontinent patients and to help restore their self-esteem, eliminate their self-imposed isolation, and allow them to
Correspondence to:
resume an active and productive lifestyle. Dr Robert D Madoff, 393 Dunlap
Street North, Suite 500, St Paul,
Faecal incontinence is a surprisingly common disorder outpatients2 found an overall prevalence of 18·4%. The MN 55104, USA
madof001@ umn.edu
that receives little attention in general and medical prevalence was twice as high for patients visiting a
publications. It can contribute to medical morbidity gastroenterologist (26·0%) as for those seeing a
(such as urinary-tract infections and decubitus ulcers) primary-care physician (13·4%). The US data, stratified
and can burden patients with substantial, continuous by frequency of episodes, showed that incontinence
financial expenses,1 but its main effect is on quality of occurred daily in 2·7% of patients, weekly in 4·5%, and
life. Patients with faecal incontinence suffer monthly or less in 7·1%. Symptomatic faecal
embarrassment, shame, and sometimes depression; incontinence occurs in 21% of women presenting with
some must plan their life around maintaining easy and urinary incontinence, pelvic-organ prolapse, or both.7
rapid access to a toilet. Not uncommonly, patients Faecal incontinence disproportionately affects
curtail or even entirely avoid activities that other individuals with severe physical and mental disabilities.
members of society take for granted: shopping, going to Patients living in institutions have an extremely high
the cinema, dining out, or having sexual intercourse. rate of faecal incontinence. Poor functional status,
Sadly, many of these lifestyle limitations are impaired cognitive ability, and limited mobility all
unnecessary, because most cases of faecal incontinence contribute to incontinence in nursing-home residents,8
are treatable. Barriers to treatment include the and the rates of incontinence rise with the length of
unwillingness of patients to broach the subject with time spent in nursing homes.9 A Canadian study of
health-care providers because of embarrassment or lack long-term hospital patients found a prevalence of 46%.10
of knowledge about the availability of treatment. Even Similarly, in a US survey of patients in nursing homes,
worse, many health-care providers are similarly reticent 47% had faecal incontinence.3 One explanation for these
or ignorant. strikingly high proportions is the advanced age, severe
debility, and numerous associated medical problems of
Epidemiology this population. However, another explanation could be
Faecal incontinence is the involuntary loss of rectal that faecal incontinence affecting a child or parent
contents through the anal canal. The true prevalence is simply cannot be managed by most families and that its
unknown, owing to the lack of standard definitions development generally mandates nursing-home
based on severity and frequency, differences in data placement. Two studies of older patients (one focused
collection, under-reporting of symptoms by patients, on patients in nursing homes, the other on those living
and variations in the populations sampled. International at home) found an association between severe faecal
population-based studies have provided widely varying incontinence and increasing mortality.9,11
estimates of prevalence, ranging from 0·004% to 18%.2–6 Under-reporting of symptoms by patients is a major
A US telephone survey found a prevalence of 2·2%; of reason for undertreatment. Only a third of symptomatic
the people who reported symptoms, 30% were over 65 patients in the USA discuss their faecal incontinence
years old and 63% were female.5 Most reported clinical with their physicians.2 In the United Arab Emirates,
series have a substantial predominance of female 60% of multiparous women with faecal incontinence do
patients, but epidemiological studies tend to show an not seek medical advice because of embarrassment, the
equal sex distribution. The reason for this discrepancy is
not known, but it might relate partly to the age and sex
Search strategy and selection criteria
of individuals who actively seek treatment.
The prevalence of faecal incontinence strongly MEDLINE was used to search for articles related to faecal
depends on the population studied. In Switzerland,7 the incontinence, emphasising those published from January,
prevalence was 4·4% in the community, 5·6% for 1998. The Cochrane Database of Systemic Reviews was also
general outpatients, 6·7% for antenatal patients, and queried for reviews related to faecal incontinence.
15·9% for urogynaecology patients. A US study of
www.thelancet.com Vol 364 August 14, 2004 621
For personal use. Only reproduce with permission from Elsevier Ltd
Review
account for much of the faecal incontinence seen in
Puborectalis men. Lateral internal sphincterotomy,22,23 fistulotomy,22
haemorrhoidectomy, and anal dilation can all result in
Rectum incontinence.24,25 Sphincter-sparing colorectal resections
can also produce incontinence, because of loss of the
X-section
rectal reservoir and stretching of the sphincter during
Anus surgery.26,27 Isolated degeneration of the internal anal
Pelvis
sphincter has been reported as a cause of soiling in both
Sacrum men and women.28
Rectum
Physical examination significantly underestimates the
frequency of postpartum sphincter disruption.29 Occult
Internal
sphincter sphincter defects have been detected by ultrasonography
External in up to 35% of primiparous women after normal
sphincter
vaginal delivery; the associated incontinence rate has
Puborectalis
ranged from 13% to 23%.30,31 More recent reports
Internal sphincter
indicate a lower rate of sphincter defects, 8–16%, with
External sphincter
little or no evidence of incontinence in the immediate
postpartum period.32,33
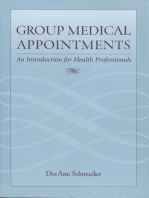
Figure 1: The anal sphincter complex A meta-analysis of 717 vaginal deliveries found a
frequency of sphincter defects of 26·9% in primiparous
hope that the problem will resolve spontaneously, the women and a frequency of new sphincter defects of
assumption that faecal incontinence is normal, or low 8·5% in multiparous women.34 Although only 29·7% of
expectations of medical care.12 sphincter defects were symptomatic in the postparum
period, the probability of faecal incontinence resulting
Aetiology from these defects was calculated to be 76·8–82·8%.
The anal sphincter complex consists of the internal and Disruption of the sphincter complex is associated with
external anal sphincter and the puborectalis muscle diminished sphincter pressures,33 and defects occur
(figure 1).13 The smooth muscle of the internal anal more frequently in women who have undergone forceps
sphincter has autonomic innervation and contributes delivery.30,32,35 Other risk factors for incontinence in
about 55% of the resting tone of the anal canal.14 The women include undergoing the first delivery, giving
external anal sphincter is a striated muscle that has a birth to a baby weighing over 4 kg, and delivering a baby
predominance of slow-twitch, fatigue-resistant muscle who is in the occiput posterior position.36 Postal surveys
fibres.15 It is continuously active and provides 20–30% of of postpartum women have reported incontinence rates
the anal resting tone;14 the remainder is provided by of 9·6% to 17·0%,37,38 with up to 50% of women having
expansion of the anal vascular cushions.14,16 The external faecal urgency or incontinence after third-degree
anal sphincter and puborectalis muscle function as one obstetric lacerations.36,39
unit, bring about voluntary sphincter contraction, and Traction injury to the pudendal nerve commonly
normally double the sphincter pressure of the anal canal accompanies obstetric sphincter laceration and
during voluntary contraction.17 The external anal contributes to faecal incontinence.40 The injury is caused
sphincter is innervated by the inferior branch of the by descent of the perineal floor, which stretches the
pudendal nerve, which emerges from Alcock’s canal on nerve as it emerges from its fixed site of exit from
the medial aspect of the ischium and traverses the Alcock’s canal. The result is muscle denervation and
ischiorectal fossa. The puborectalis muscle is also subsequent reinnervation by nerve sprouting.41 An
directly innervated by the S3 and S4 sacral nerves.18,19 identical neuropathy causes incontinence in patients
Sensation is provided by receptors in the pelvic floor that with rectal prolapse,42 chronic straining at stool,43,44 and
detect rectal distension20 and by various receptors in the pelvic-floor descent.44
anal transition zone.20,21 Faecal impaction is an important cause of
Congenital malformations such as imperforate anus, incontinence, particularly in older people and those
rectal agenesis, and cloacal defect all can cause faecal living in institutions. Impaction-associated overflow
incontinence. The severity depends on the bulk and incontinence has generally been attributed to chronic
development of pelvic-floor muscles and the degree of reflex inhibition of the internal anal sphincter, but
impairment of sensory mechanisms. physiological studies have shown that the cause is a
A greater proportion of cases of faecal incontinence combination of decreased anorectal sensation and
are acquired. Sphincter disruption resulting from reduced sphincter pressures. Factors contributing to
vaginal delivery is the most common sphincter injury. impaction include inadequate fibre and water intake,
Other causes of anatomical defects, including anorectal metabolic disorders (hypercalcaemia, hypokalaemia,
surgery and trauma from impalement or pelvic fracture, hypothyroidism), immobility, dementia, depression, and
622 www.thelancet.com Vol 364 August 14, 2004
For personal use. Only reproduce with permission from Elsevier Ltd
Review
drugs (eg, narcotics, antipsychotics, antidepressants, Panel: Causes of incontinence
diuretics, and calcium-channel blockers).45
Despite the importance of adequate pelvic-floor Congenital
function, maintenance of continence depends on an Imperforate anus
intact chain of anatomical structures and physiological Rectal agenesis
mechanisms, a sequence extending from the anus to the Cloacal defects
brain. Patients must have the awareness and desire to Myelomeningocele
maintain continence. Many patients with dementia are Meningocele
incontinent because of a lack of interest in, or awareness Anatomical
of, bowel function. Neurological disease or injury that Obstetric injury, vaginal delivery
affects the brain, spinal cord, or peripheral nerves can Anorectal surgery
cause incontinence. Congenital neurological causes Sphincter-sparing bowel resection
include spina bifida, myelomeningocele, and Pelvic fracture
meningocele. Acquired neurological causes include Anal impalement
stroke, tumours, spinal-cord injury, multiple sclerosis,
and diabetic autonomic neuropathy. Neurological
Abnormal gastrointestinal function can also cause Diabetes mellitus
faecal incontinence. Excessive stool volume and rapid Multiple sclerosis
gut transit can overwhelm an entirely normal pelvic Stroke
floor. Contributory abnormalities include intestinal Dementia
malabsorption, inflammatory bowel disease, and Central nervous system tumour, infection, trauma
infectious diarrhoea. Spina bifida
Finally, we should emphasise that in many cases Pudendal neuropathy
faecal incontinence arises from a combination of Functional
factors. Pudendal neuropathy commonly accompanies Psychiatric disorder
obstetric sphincter injury, as already noted. Similarly, Malabsorption
women with pre-existing irritable bowel syndrome have Inflammatory bowel disease
more postpartum defecatory urgency and incontinence Radiation proctitis
to flatus than those without, despite a similar frequency Hypersecretory tumours
of sphincter injury.46 The fact that many women with Rectal intussusception, prolapse
sphincter injuries do not develop incontinence until Faecal impaction
later in life also suggests a cumulative, multifactorial Physical disabilities
process. The possible causes of incontinence are
summarised in the panel.
infrequent loss of solid stool.47 The degree of
Assessment incontinence can also be inferred from the patient’s use
Many patients find the subject of faecal incontinence of pads or other protection and from restrictive changes
difficult to discuss, so they may provide limited or in lifestyle, but these behavioural factors may be more
misleading information. Common complaints include strongly influenced by the patient’s anxiety than the
urgency, pruritus (which is caused by soiling), and actual severity of the disorder. Incontinence can be
“diarrhoea,” a term commonly used by patients to classified into two categories on basis of the history:
denote incontinence. Clinicians eliciting such passive (unconscious loss of stool) and urge (inability to
complaints should investigate further, particularly if the control a perceived impending bowel movement).48
patient’s history (eg, recent vaginal delivery) or physical Many patients with physical and psychological
findings suggest faecal incontinence. True incontinence impairments have faecal incontinence, so assessment of
must be differentiated from perineal soiling due to the patient’s functional status is important. Physical
inadequate hygiene or prolapsing haemorrhoids. disabilities can impede access to a toilet, preclude
transfer to or sitting on a commode, or prevent cleaning
History up after bowel movements. Cognitive impairment can
When taking the history, clinicians should attend to affect the ability to sense the need to defecate or the
these essential elements: the onset and type of desire to defecate in a controlled way. Environmental
incontinence (flatus, liquid, or solid stool); the frequency assessment in some cases uncovers contributory factors
of episodes; and any related changes in bowel function to incontinence, such as a lack of accessible toilets.
or stool consistency. Solid stool is easier to control than
liquid, so the loss of solid stool generally indicates a Scoring systems
greater degree of physiological impairment. However, Planning of treatment and assessment of the results
loss of liquid stool is more troublesome to patients than requires a judgment of the severity of incontinence. In
www.thelancet.com Vol 364 August 14, 2004 623
For personal use. Only reproduce with permission from Elsevier Ltd
Review
Normal appearance systems compared in one study correlated with the
physician’s clinical impression.50,52
Several issues must be resolved before an ideal scoring
system is developed: the definition of incontinence must
be standardised; the optimum method of data collection
must be decided on (ie, diary versus patients’ recall); the
need for data beyond type and frequency must be
assessed; and the assignment of numerical values to the
combinations of type and frequency must be validated.
The developers of the faecal incontinence severity index
used patients’ input to assign numerical values, but
further work is necessary.47,50 Interpretation of
publications on incontinence is difficult because of the
lack of standardisation, and even more important,
because various methods are used for data collection.
External sphincter defect For example, maintenance of a daily diary of bowel
movements is a far more stringent method than
patients’ recall, so results of treatment may appear to be
worse. Even the diary approach is limited by the
confounding factor of the patient’s activity: the most
severely affected patient can appear continent by
refusing to venture from a nearby toilet.
Quality of life should be assessed independently of
severity, because the two measures do not necessarily
correlate. Overall health-status instruments and
gastrointestinal quality-of-life instruments have been
used to measure quality of life related to faecal
incontinence, with mixed results.53,54 A recently validated
incontinence-specific quality-of-life scale measures four
variables (lifestyle, coping/behaviour, depression/self-
Internal sphincter defect perception, and embarrassment); it is more sensitive
than global scales.55
Physical examination
Physical examination reveals the cause of the
incontinence in many cases. Pertinent findings include
a thinned or deformed perineal body and scars from
previous surgery or trauma. Breakdown of the perianal
skin is a consequence, not a cause of incontinence, but
skin condition should be noted and addressed. Gaping
of the anus suggests rectal prolapse, which can usually
be demonstrated with Valsalva’s manoeuvre. Digital
rectal examination can be used to diagnose faecal
impaction associated with overflow incontinence; such
an examination is essential to exclude tumours in the
Figure 2: Endoanal ultrasonography
anal canal or low rectum. Furthermore, the examiner
can assess both resting anal-sphincter tone and the
patient’s ability to augment it with voluntary squeeze
contrast to many other disorders, no physiological index effort. Diminished perianal sensation and the absence
of faecal incontinence accurately reflects clinical of an anal wink suggest a neurogenic cause of
severity.49 That fact led to the development of scoring incontinence.
systems based on patients’ reports of symptoms.50 The Endoscopy to exclude a mass or inflammatory
most widely used system includes as variables the condition is a key adjunct to the physical examination.
frequency and type of incontinence, the extent of Flexible sigmoidoscopy is adequate in most cases, but
lifestyle changes, and the need to wear a pad.51 Although complete colonoscopy should be done if the patient has
none of the currently used scoring systems has been unexplained diarrhoea, bleeding, or changed bowel
psychometrically validated, the scores with all four habits. The patient’s ability to retain a 100 mL water
624 www.thelancet.com Vol 364 August 14, 2004
For personal use. Only reproduce with permission from Elsevier Ltd
Review
enema is a useful bedside measure of sphincter
function.
Anorectal physiology testing
Testing of anorectal physiology is useful both as a
diagnostic tool and as a way to quantify the magnitude
of the physiological defect. Such testing is particularly
important when the results of the physical examination
are normal, when rectal prolapse is suspected but not
demonstrable, or when surgery is contemplated. Useful
laboratory studies include endoanal ultrasonography,
anal manometry, electromyography, and defecography.
Imaging
Endoanal ultrasonography is a simple and rapid
technique that permits accurate delineation of anal-
sphincter anatomy (figure 2). When done by an
experienced ultrasonographer, the method has
sensitivity and specificity of almost 100% in identifying
defects of the internal and external sphincter.56 It can
also reveal unsuspected sphincter injuries in a patient
thought to have neurogenic incontinence or rule out
significant anatomical pathology in a patient with
suspected sphincter disruption; either result might lead
to a change in the planned therapy.57 Sphincter
abnormalities are shown on endoanal ultrasonography
in up to 90% of women whose sole risk factor for faecal
incontinence is obstetric trauma; thus, this imaging
technique is essential for complete assessment of
incontinent parous women.
MRI is another approach to pelvic-floor imaging
(figure 3).58 The need for an endoanal coil to optimise
imaging remains controversial. Advantages of MRI
include lower dependency on the operator, a wider field
of view, and the ability to undertake dynamic studies of
pelvic-floor function. Endoanal ultrasonography and
MRI have similar accuracy in diagnosing defects of the
external anal sphincter, but endoanal ultrasonography is
more accurate in diagnosing injuries of the internal anal
sphincter.59
Manometry
Anal manometry assesses function of the internal and
external anal sphincter, the rectoanal inhibitory reflex,
and rectal sensation. It uses a microballoon, a water-
perfused catheter, or a solid-state transducer. In a Figure 3: MRI of the normal pelvis
relaxed patient, resting pressures mainly reflect function Sagittal phased-array images of the anal canal and perianal structures.
AC=anococcygeal body; BS=bulbospongiosus; EAS=external anal sphincter;
of the internal anal sphincter; squeeze pressures PB=perineal body; PU=pubic bone. Reprinted with permission.58
represent voluntary contraction of the external anal
sphincter. Normal values of both resting and squeeze
pressures vary among patients: they are lower in women incontinent patients will not necessarily correct
than men and in older patients of both sexes.17 Despite a manometric abnormalities, and in fact it commonly
general relation between sphincter pressure and does not.
continence, sphincter pressure varies substantially in The rectoanal inhibitory reflex causes relaxation of the
both continent and incontinent populations.17,49 That fact internal anal sphincter in response to rectal distension.
helps emphasise the multifactorial nature of It is demonstrated by a drop in resting anal pressure in
incontinence. Furthermore, successful treatment of response to inflation of a rectal balloon. This reflex could
www.thelancet.com Vol 364 August 14, 2004 625
For personal use. Only reproduce with permission from Elsevier Ltd
Review
Neurophysiological tests
Faecal incontinence History and physical Diarrhoea? Neurophysiological assessment of incontinent patients
examination is done by single-fibre electromyography or pudendal-
nerve terminal motor latency (PNTML) testing. Single-
Yes No
• Assess/treat aetiology of diarrhoea: colitis, hypersecretory fibre electromyography shows multiphasic action
tumour, radiation, overflow potentials in the external anal sphincter, a finding
• Medical treatment: fibre, dietary, barrier cream, antidiarrhoeal diagnostic of muscle denervation and subsequent
agents, bowel regimen
Anorectal physiology testing reinnervation.41 Although it provides more direct
• Anorectal manometry
• Pudendal nerve testing
evidence of denervation, single-fibre electromyography
Improves
Does not • Endoanal ultrasonography has largely been supplanted in many centres by PNTML
resolve • Defecography (optional) testing, which uses a glove-mounted intra-anal electrode
rather than a needle electrode.66 PNTML testing
Sphincter defect? measures conduction time from stimulation of the
nerve at the ischial spine to contraction of the external
Yes No anal sphincter. Because PNTML testing measures
Major defect? conduction time in the fastest remaining nerve fibres,
significant nerve damage is sometimes overlooked.
Yes No Results are also influenced by the patient’s body type
Biofeedback and the technician’s expertise.67 Long latencies are
Overlapping associated with traction injury to the nerve as well as
sphincteroplasty with primary neuropathies. Pudendal neuropathy is
seen in up to 70% of patients with faecal incontinence,
Improves Fails
and in more than 50% of patients with sphincter
Improves Fails
injury.68 Some investigators have related the presence of
pudendal neuropathy to poor results after
Endoanal ultrasonography: sphincteroplasty,69 but others have not been able to
persistent sphincter defect? Consider indications, demonstrate an association.70 Enthusiasm for PNTML
age, comorbidities,
Yes No technical issues testing has been tempered by the lack of consensus
about its accuracy and predictive value for outcome after
Repeat sphincteroplasty with surgery.
or without biofeedback
Dynamic graciloplasty Defecography
Artifical sphincter Defecography examines rectal emptying of a soft barium
Improves Fails Sacral stimulation Stoma
paste under fluoroscopy. Although useful for
assessment of patients with obstructed defecation, it has
limited value in most incontinent patients. Its main role
Figure 4: Algorithm for incontinence in patients with faecal incontinence is to help diagnose
occult rectal prolapse or other suspected pelvic-floor
abnormalities (such as a poorly emptying rectocele).
permit “sampling” of the rectal contents by the
transitional-zone receptors, a process that assists in the Treatment
decision to initiate or defer defecation. The exact Medical therapy
mechanism of the decision process remains uncertain. An algorithm for the treatment of incontinence is given
This reflex is absent in patients with Hirschsprung’s in figure 4. Initial treatment should be conservative.
and Chagas’ diseases; its loss after low rectal Dietary changes (eg, avoidance of foods that cause
anastomosis is associated with poor functional diarrhoea or urgency), the addition of supplementary
outcome.60 fibre, and bowel habit training are useful for most
Rectal sensory testing includes volumetric patients. They may even be the only treatment necessary
measurements of the first detectable sensation, the for those with mild incontinence. Barrier creams, cotton
sensation of fullness, and the maximum tolerated wicks at the anus, and rectal washouts can prevent or
volume by balloon distension. Hypersensitivity can be ameliorate anal excoriation secondary to leakage. In
seen with inflammatory disorders, after irradiation, and patients with diarrhoea, assessment of the cause and
with irritable bowel syndrome;61 it can lead to urge specific treatment directed at the underlying cause are
incontinence. Blunted sensation can also contribute to needed. Patients with idiopathic diarrhoea are treated
incontinence;62,63 it is associated with megarectum and with antidiarrhoeal medications, such as loperamide,
with neurogenic disorders such as diabetes and multiple diphenoxylate, and bile-acid binders. Loperamide
sclerosis.64,65 decreases intestinal motility and secretion and increases
626 www.thelancet.com Vol 364 August 14, 2004
For personal use. Only reproduce with permission from Elsevier Ltd
Review
sphincter pressure.71 Bulking agents, such as psyllium medical and nursing care (advice) or advice plus
compounds, are also used, because control of solid stool sphincter exercises.96
is easier than control of liquid stool. Conversely, patients Many issues about biofeedback remain unresolved. It
with constipation and faecal impaction may need is not uniformly available and not covered by all health
routine enemas or laxatives to empty the rectum, so that insurance schemes. No clear criteria for selection of
overflow incontinence does not occur. Incontinent patients have been identified. The optimum protocol,
patients with associated irritable bowel syndrome equipment, and duration of treatment are unknown.
present a therapeutic challenge, given their alternating The mechanism of improvement is poorly understood.
symptoms of diarrhoea and constipation. No consistent change in sphincter pressures, rectal
Novel approaches to the medical treatment of sensation, or duration of contraction has been reported.
incontinence include oestrogen replacement therapy in Long-term follow-up data are limited, albeit promising,
postmenopausal women,72 amitriptyline,73 and valproate in a few small studies.97–99
sodium.74 Topical 10% phenylephrine increased resting
anal pressure in healthy volunteers75 and improved Surgery
seepage in patients with ileoanal reservoirs,76 but it was To restore the anal aperture by repairing sphincter
ineffective in a randomised controlled trial of defects is the cornerstone of surgery for incontinence.
incontinent patients.77 At the time of a recognised obstetric injury, immediate
direct repair is advocated, yet persistent defects are
Biofeedback common.29,35,100 If immediate repair is not attempted,
Biofeedback is commonly the first treatment patients should wait at least 3 months before surgery, so
recommended if medical therapy fails. It is appealing that the magnitude of the functional deficit can be
because it is simple, cheap, and without adverse physical defined, physiological assessment can be done, and local
effects. The goal is improved contraction of the external tissue inflammation and oedema can resolve.
anal sphincter in response to rectal distention. Various
protocols and feedback equipment have been Sphincteroplasty
reported.78–86 In general, three different protocols are Established injuries in symptomatic patients are treated
used: coordination training, which teaches patients to by overlapping sphincteroplasty. In this technique, a
contract the sphincter muscle in response to rectal curvilinear incision is made over the perineal body, and
distension; sensory training, which teaches patients to the scarred sphincter remnant is dissected back to
recognise progressively smaller volumes of rectal healthy muscle on either side. The scar is transected, but
distension; and strength training, which teaches not excised, and is used as part of the overlapping repair
patients to isolate and exercise the sphincter muscle to restore an intact ring of muscle. Many surgeons
without using rectal distension. The length and the plicate the levator muscles anteriorly, in an effort to add
number of sessions recommended vary widely. In most length to the restored anal canal, but no objective data
centres, manometry equipment or an electromyographic support this approach. Other surgeons avoid levator-
rectal probe is used to provide information to patients. muscle plication out of fear of causing dyspareunia.
The technique chosen does not seem to affect the Individual repair of the internal and external anal
likelihood of success.87 sphincter has been advocated by some researchers, but it
Success rates after biofeedback range from 38% to is not widely practised; moreover, proof of its superiority
100%.64,78,88–90 The presence of a sphincter defect limits to single-layer repair is lacking.101 Routine sphinctero-
but does not preclude the possibility of a good plasty is generally done without creation of a diverting
response.90 Pudendal neuropathy does not adversely stoma; randomised trials have shown no benefit from
affect clinical outcome,91,92 though poor results have been diversion and morbidity was increased.102,103
reported in patients with severe neurogenic faecal As with all therapies for incontinence, the reported
incontinence who lack rectal sensation.93 The reported success of sphincteroplasty depends on the definitions
success rates for coordination training and for strength of incontinence and on the data-collection method. Still,
training do not differ significantly. most series report that 60–88% of patients achieve an
Interpretation of reports on biofeedback is difficult. excellent or good outcome, defined as perfect continence
Most studies have been retrospective. Parallel design or as incontinence to flatus with minor staining.69,70,104–106
and randomisation have rarely been used. The definition About 15–20% experience no change or a worse
of success varies widely, and follow-up is short. In most outcome. However, several studies have shown that the
studies, the sample size is small and criteria for results of sphincteroplasty deteriorate substantially with
selection of patients are not reported. Few studies time.105,107–109
include controls.78,94 Studies comparing biofeedback with Some69,106,109,110 but not all series69,103,108 suggest that the
attentive medical care alone are rare and have given presence of pudendal neuropathy adversely affects the
conflicting results.88,95 However, a randomised controlled outcome of overlapping sphincter repair. Patients for
trial showed no advantage of biofeedback over standard whom sphincteroplasty fails should undergo follow-up
www.thelancet.com Vol 364 August 14, 2004 627
For personal use. Only reproduce with permission from Elsevier Ltd
Review
ultrasonography to ensure that the muscle wrap is remains an option for refractory incontinence in a
intact; patients with persisting defects can undergo limited number of centres, but it is not approved for use
repeat repair after 6–12 months.111,112 Biofeedback can be in the USA.
effective salvage therapy for patients with suboptimum The artificial anal sphincter (Acticon Neosphincter,
results after sphincteroplasty.91 American Medical Systems, Minneapolis, MN, USA)
maintains continence via a fluid-filled cuff that
Diversion surrounds and compresses the anal canal. The patient
If all other therapies have failed or if comorbidities controls the device via a pump placed in the scrotum or
preclude more aggressive therapy, faecal diversion labia majora. Squeezing the pump nine to 12 times
remains an excellent alternative. Many patients express forces the fluid from the cuff into a reservoir balloon,
reluctance to live with a stoma, but counselling by the which is implanted behind the pubic bone in
physician and an enterostomal therapist can be preperitoneal tissues. Once the cuff is deflated, the anal
persuasive. Colostomy admittedly does not confer canal is open, allowing the passage of stool. The cuff
continence, but it does restore control of bowel then gradually reinflates to occlude the anal canal until
evacuation and permits resumption of a normal defecation is again desired.
personal and social life. Emphasis should be placed on Christiansen and Lorentzen first reported
creating a well-constructed stoma at an appropriate site, implantation of an artificial anal sphincter for faecal
to limit difficulty with its management. incontinence in 1987.118 Since then, variable results with
the technique have been reported.119–124 Lehur and
Innovations colleagues reported successful results in 75% of
Restoration of continence to patients when traditional patients, with 29% requiring at least temporary removal
treatment fails, or when traumatic or neurogenic of the device.123 By contrast, Malouf and co-workers
injuries are extensive, remains a challenge. Even after reported successful results in only 38% of patients;
an initial successful result with biofeedback or anterior infection, particularly with meticillin-resistant
sphincteroplasty, only about 50% of patients retain the Staphylococcus aureus, was the major cause of failure.124
post-treatment degree of continence for 3 years or In a multicentre clinical trial, 67% of patients had a
longer.97,106,108 Options available to such patients include functional device in place at 1 year postoperatively.125
dynamic graciloplasty, an artificial anal sphincter, and The mean incontinence score (range 0–120) dropped
sacral-nerve stimulation. from 105 (incontinent to liquids and solids daily) to 48
Dynamic graciloplasty and artificial anal sphincters (seepage). The infection rate necessitating surgical
are advanced variations of anal encirclement. The revision was 25%. In all, 46% of patients (51 of 112)
earliest and simplest version of anal encirclement was required surgical revision; 37% (41 of 112) required
the use of silver wire, described by Thiersch in 1891. device removal, seven of whom (17%) underwent
Later, Pickrell and colleagues described anal successful reimplantation.
encirclement by use of the gracilis muscle, and other The artificial anal sphincter is suitable for many of the
researchers have favoured use of gluteal-muscle flaps.113 same patients who are candidates for dynamic
Functional results with passive muscle wraps are graciloplasty. However, the perineal soft tissue must be
limited by the inability of patients to maintain, at all sufficient to allow placement of a Silastic cuff around
times, continuous voluntary contraction of the muscle. the anal canal. The device is now available in Europe,
Dynamic graciloplasty combines transposition of the Canada, and the USA.
gracilis muscle with electrical stimulation via an Sacral-nerve stimulation, like the artificial anal
implantable pulse generator. Application of graded sphincter, was initially devised for urinary incontinence.
electrical stimulation allows conversion of the fast- Matzel and colleagues introduced the use of such
twitch, fatiguable gracilis muscle to a slow-twitch, stimulation in 1995 to treat patients with functional, but
fatigue-resistant muscle that more closely resembles the not anatomical, deficits of the anal sphincter muscle.126
anal sphincter.114 The procedure entails placing an electrode in a sacral
Baeten and co-workers first reported the use of foramen (generally S3) to stimulate the sacral nerves.
electrical stimulation with a gracilis-muscle wrap for The desired effect is maximum contraction of pelvic
faecal incontinence in 1988115 and subsequently muscles, with the minimum possible stimulation of the
reported a 72% continence rate. However, multicentre fibres to the leg. Once the optimum site has been
studies have been unable to replicate this degree of selected, the lead is connected to a temporary external
success without substantial morbidity and high pulse generator for 2 weeks of test stimulation. If
reoperation rates.116,117 This discrepancy appears to arise function improves adequately, a permanent pulse
at least partly from a relative lack of experience with the generator is implanted. Both the initial operation for
technique. Surgeons new to the operation have higher lead placement and the subsequent one for placement of
morbidity rates and lower success rates than those with the pulse generator are done under local anaesthesia
substantial experience.116 Dynamic graciloplasty with conscious sedation.
628 www.thelancet.com Vol 364 August 14, 2004
For personal use. Only reproduce with permission from Elsevier Ltd
Review
Recent series of patients treated by sacral-nerve Medical Systems, manufacturer of the Acticon Neosphincter artificial
stimulation have shown promising results with little bowel sphincter. None of the authors received payment (except from
The Lancet) for writing this review.
morbidity.127,128 Success rates after short-term stimulation
approach 90%.129 The great majority of patients for whom Acknowledgments
We thank Alexandra A Broek for assistance in preparation of the review,
test stimulation is successful remain continent after and Mary E Knatterud for editorial help.
permanent implantation.127,130–132 However, infection and
References
lead displacement remain challenging in up to 25% of 1 Mellgren A, Jensen LL, Zetterstrom JP, Wong WD, Hofmeister JH,
patients.133 Because of continuing pain, device reposi- Lowry AC. Long-term cost of fecal incontinence secondary to
tioning or explantation has been needed for several obstetric injuries. Dis Colon Rectum 1999; 42: 857–65.
2 Johanson JF, Lafferty J. Epidemiology of fecal incontinence: the
patients.127,130 silent affliction. Am J Gastroenterol 1996; 91: 33–36.
Most studies of sacral-nerve stimulation have shown 3 Nelson R, Furner S, Jesudason V. Fecal incontinence in Wisconsin
improvement in both resting and squeeze anal nursing homes: prevalence and associations. Dis Colon Rectum
1998; 41: 1226–29.
pressures as well as increased rectal sensation.133
4 Thomas TM, Egan M, Walgrove A, Meade TW. The prevalence
Ambulatory manometry has shown reduced rectal of faecal and double incontinence. Community Med 1984; 6:
contractility and suppression of spontaneous anal 216–20.
relaxation.129 The mechanism by which these effects are 5 Nelson R, Norton N, Cautley E, Furner S. Community-based
prevalence of anal incontinence. JAMA 1995; 274: 559–61.
mediated remains uncertain, though many researchers 6 Drossman DA, Li Z, Andruzzi E, et al. US householder survey of
believe that sacral-nerve stimulation works by functional gastrointestinal disorders: prevalence, sociodemography,
modulating local reflex arcs. The mechanism could well and health impact. Dig Dis Sci 1993; 38: 1569–80.
be multifactorial. Sacral-nerve stimulation is available in 7 Faltin DL, Sangalli MR, Curtin F, Morabia A, Weil A. Prevalence of
anal incontinence and other anorectal symptoms in women.
Europe; in the USA, qualifying patients with faecal Int Urogynecol J Pelvic Floor Dysfunct 2001; 12: 117–20.
incontinence can enrol in a trial approved by the Food 8 Porell F, Caro FG, Silva A, Monane M. A longitudinal analysis of
and Drug Administration. nursing home outcomes. Health Serv Res 1998; 33: 835–65.
9 Chassagne P, Landrin I, Neveu C, et al. Fecal incontinence in the
Recent work has investigated novel minimally invasive institutionalized elderly: incidence, risk factors, and prognosis.
approaches to faecal incontinence. One option, the Am J Med 1999; 106: 185–90.
addition of a bulking agent to the anal canal to augment 10 Borrie MJ, Davidson HA. Incontinence in institutions: costs and
contributing factors. CMAJ 1992; 147: 322–28.
resting tone, stems from the routine use of bulking
11 Nakanishi N, Tatara K, Shinsho F, et al. Mortality in relation to
agents for treatment of urinary incontinence caused by urinary and faecal incontinence in elderly people living at home.
intrinsic urinary-sphincter deficiency. The successful Age Ageing 1999; 28: 301–06.
use of implantable microballoons,134 carbon-coated 12 Rizk DE, Hassan MY, Shaheen H, Cherian JV, Micallef R, Dunn E.
The prevalence and determinants of health care-seeking behavior
beads,135 autologous fat,136 silicone,137 and collagen138 have for fecal incontinence in multiparous United Arab Emirates
each been reported in small series with low morbidities. females. Dis Colon Rectum 2001; 44: 1850–56.
However, both the magnitude and the durability of 13 Jorge JM. Anorectal anatomy and physiology. In: Wexner SD, ed.
Fundamentals of anorectal surgery, 2nd edn. Philadelphia:
improvement have varied with such techniques.139 A W B Saunders, 1998: 1–24.
second investigational approach has used radio- 14 Lestar B, Penninckx F, Kerremans R. The composition of anal basal
frequency energy to apply a series of small submucosal pressure: an in vivo and in vitro study in man. Int J Colorectal Dis
1989; 4: 118–22.
burns to the anal canal. A pilot series showed promising
15 Johnson MA, Polgar J, Weightman D, Appleton D. Data on the
results,140 but a larger trial showed a lesser degree of distribution of fibre types in thirty-six human muscles: an autopsy
improvement.141 study. J Neurol Sci 1973; 18: 111–29.
16 Gibbons CP, Trowbridge EA, Bannister JJ, Read NW. Role of anal
cushions in maintaining continence. Lancet 1986; 1: 886–88.
Conclusion 17 McHugh SM, Diamant NE. Effect of age, gender, and parity on anal
Faecal incontinence is an embarrassing and sometimes canal pressures: contribution of impaired anal sphincter function to
debilitating disorder. Although incontinence is generally fecal incontinence. Dig Dis Sci 1987; 32: 726–36.
18 Matzel KE, Schmidt RA, Tanagho EA. Neuroanatomy of the striated
treatable, many patients remain untreated because they muscular anal continence mechanism: implications for the use of
do not report their symptoms or because their health- neurostimulation. Dis Colon Rectum 1990; 33: 666–73.
care provider is not familiar with available treatment 19 Snooks SJ, Swash M. The innervation of the muscles of continence.
options. Conservative therapy is successful for many Ann R Coll Surg Engl 1986; 68: 45–49.
20 Parks AG. Anorectal incontinence. Proc R Soc Med 1975; 68:
cases of mild incontinence, but more severe cases 681–90.
should be formally assessed before treatment is 21 Duthie HL, Gairns FN. Sensory nerve endings and sensation in the
undertaken. Recent advances have provided new anal region of man. Br J Surg 1960; 47: 585–95.
therapeutic options for patients with refractory 22 Garcia-Aguilar J, Belmonte C, Wong WD, Lowry AC, Madoff RD.
Open vs closed sphincterotomy for chronic anal fissure: long-term
incontinence. results. Dis Colon Rectum 1996; 39: 440–43.
Conflict of interest statement 23 Nyam DC, Pemberton JH. Long-term results of lateral internal
Robert D Madoff consults for Medtronic, manufacturer of the hardware sphincterotomy for chronic anal fissure with particular reference to
used for dynamic graciloplasty and sacral-nerve stimulation, and for incidence of fecal incontinence. Dis Colon Rectum 1999; 42:
1306–10.
Solvay Pharmaceuticals, manufacturer of topical phenylephrine
hydrochloride. Susan C Parker consults for Medtronic and for American 24 MacIntyre IM, Balfour TW. Results of the Lord non-operative
treatment for haemorrhoids. Lancet 1972; 1: 1094–95.
www.thelancet.com Vol 364 August 14, 2004 629
For personal use. Only reproduce with permission from Elsevier Ltd
Review
25 Read MG, Read NW, Haynes WG, Donnelly TC, Johnson AG. A 50 Baxter NN, Rothenberger DA, Lowry AC. Measuring fecal
prospective study of the effect of haemorrhoidectomy on sphincter incontinence. Dis Colon Rectum 2003; 46: 1591–605.
function and faecal continence. Br J Surg 1982; 69: 396–98. 51 Jorge JM, Wexner SD. Etiology and management of fecal
26 Otto IC, Ito K, Ye C, et al. Causes of rectal incontinence after incontinence. Dis Colon Rectum 1993; 36: 77–97.
sphincter-preserving operations for rectal cancer. Dis Colon Rectum 52 Vaizey CJ, Carapeti E, Cahill JA, Kamm MA. Prospective
1996; 39: 1423–27. comparison of faecal incontinence grading systems. Gut 1999; 44:
27 Ho YH, Tsang C, Tang CL, Nyam D, Eu KW, Seow-Choen F. 77–80.
Anal sphincter injuries from stapling instruments introduced 53 Eypasch E, Williams JI, Wood-Dauphinee S, et al. Gastrointestinal
transanally: randomized, controlled study with endoanal ultrasound quality of life index: development, validation and application of a
and anorectal manometry. Dis Colon Rectum 2000; 43: 169–73. new instrument. Br J Surg 1995; 82: 216–22.
28 Vaizey CJ, Kamm MA, Bartram CI. Primary degeneration of the 54 Sailer M, Bussen D, Debus ES, Fuchs KH, Thiede A. Quality of life
internal anal sphincter as a cause of passive faecal incontinence. in patients with benign anorectal disorders. Br J Surg 1998; 85:
Lancet 1997; 349: 612–15. 1716–19.
29 Warshaw JS. Obstetric anal sphincter injury: incidence, risk factors, 55 Rockwood TH, Church JM, Fleshman JW, et al. Fecal incontinence
and repair. Sem Colon Rectal Surg 2001; 12: 90–97. quality of life scale: quality of life instrument for patients with fecal
30 Sultan AH, Kamm MA, Hudson CN, Thomas JM, Bartram CI. incontinence. Dis Colon Rectum 2000; 43: 9–16.
Anal-sphincter disruption during vaginal delivery. N Engl J Med 56 Sultan AH, Kamm MA, Talbot IC, Nicholls RJ, Bartram CI. Anal
1993; 329: 1905–11. endosonography for identifying external sphincter defects
31 Faltin DL, Boulvain M, Irion O, Bretones S, Stan C, Weil A. confirmed histologically. Br J Surg 1994; 81: 463–65.
Diagnosis of anal sphincter tears by postpartum endosonography to 57 Liberman H, Faria J, Ternent CA, Blatchford GJ, Christensen MA,
predict fecal incontinence. Obstet Gynecol 2000; 95: 643–47. Thorson AG. A prospective evaluation of the value of anorectal
32 Varma A, Gunn J, Gardiner A, Lindow SW, Duthie GS. Obstetric physiology in the management of fecal incontinence. Dis Colon
anal sphincter injury: prospective evaluation of incidence. Rectum 2001; 44: 1567–74.
Dis Colon Rectum 1999; 42: 1537–43. 58 Morren GL, Beets-Tan RG, van Engelshoven JM. Anatomy of the
33 Zetterstrom J, Mellgren A, Jensen LL, et al. Effect of delivery on anal canal and perianal structures as defined by phased-array
anal sphincter morphology and function. Dis Colon Rectum 1999; magnetic resonance imaging. Br J Surg 2001; 88: 1506–12.
42: 1253–60. 59 Malouf AJ, Williams AB, Halligan S, Bartram CI, Dhillon S,
34 Oberwalder M, Connor J, Wexner SD. Meta-analysis to determine Kamm MA. Prospective assessment of accuracy of endoanal MR
the incidence of obstetric anal sphincter damage. Br J Surg 2003; 90: imaging and endosonography in patients with fecal incontinence.
1333–37. AJR Am J Roentgenol 2000; 175: 741–45.
35 Varma A, Gunn J, Lindow SW, Duthie GS. Do routinely measured 60 Lewis WG, Martin IG, Williamson ME, et al. Why do some
delivery variables predict anal sphincter outcome? Dis Colon Rectum patients experience poor functional results after anterior
1999; 42: 1261–64. resection of the rectum for carcinoma? Dis Colon Rectum 1995;
36 Sultan AH, Kamm MA, Hudson CN, Bartram CI. Third degree 38: 259–63.
obstetric anal sphincter tears: risk factors and outcome of primary 61 Prior A, Maxton DG, Whorwell PJ. Anorectal manometry in
repair. BMJ 1994; 308: 887–91. irritable bowel syndrome: differences between diarrhoea and
37 Faltin DL, Sangalli MR, Roche B, Floris L, Boulvain M, Weil A. constipation predominant subjects. Gut 1990; 31: 458–62.
Does a second delivery increase the risk of anal incontinence? 62 Buser WD, Miner PB Jr. Delayed rectal sensation with fecal
Br J Obstet Gynecol 2001; 108: 684–88. incontinence: successful treatment using anorectal manometry.
38 MacArthur C, Glazener CM, Wilson PD, et al. Obstetric Gastroenterology 1986; 91: 1186–91.
practice and faecal incontinence three months after delivery. 63 Gladman MA, Scott SM, Chan CL, Williams NS, Luniss PJ. Rectal
Br J Obstet Gynecol 2001; 108: 678–83. hyposensitivity: prevalence and clinical impact in patients with
39 Sorensen M, Tetzschner T, Rasmussen OO, Bjarnesen J, intractable constipation and fecal incontinence. Dis Colon Rectum
Christiansen J. Sphincter rupture in child birth. Br J Surg 1993; 80: 2003; 46: 238–46.
392–94. 64 Wald A, Tunuguntla AK. Anorectal sensorimotor dysfunction in
40 Snooks SJ, Swash M, Setchell M, Henry MM. Injury to innervation fecal incontinence and diabetes mellitus: modification with
of pelvic floor sphincter musculature. Lancet 1984; 2: 546–50. biofeedback therapy. N Engl J Med 1984; 310: 1282–87.
41 Neill ME, Swash M. Increased motor unit fibre density in the 65 Caruana BJ, Wald A, Hinds JP, Eidelman BH. Anorectal sensory
external anal sphincter muscle in ano-rectal incontinence: a single and motor function in neurogenic fecal incontinence: comparison
fibre EMG study. J Neurol Neurosurg Psychiatry 1980; 43: 343–47. between multiple sclerosis and diabetes mellitus. Gastroenterology
42 Parks AG, Swash M, Urich H. Sphincter denervation in anorectal 1991; 100: 465–70.
incontinence and rectal prolapse. Gut 1977; 18: 656–65. 66 Kiff ES, Swash M. Slowed conduction in the pudendal nerves in
43 Snooks SJ, Barnes PR, Swash M, Henry MM. Damage to the idiopathic (neurogenic) faecal incontinence. Br J Surg 1984; 71:
innervation of the pelvic floor musculature in chronic constipation. 614–16.
Gastroenterology 1985; 89: 977–81. 67 Yip B, Barrett RC, Coller JA, et al. Pudendal nerve terminal motor
44 Kiff ES, Barnes PR, Swash M. Evidence of pudendal neuropathy in latency testing: assessing the educational learning curve: can we
patients with perineal descent and chronic straining at stool. Gut teach our own? Dis Colon Rectum 2002; 45: 184–87.
1984; 25: 1279–82. 68 Roig JV, Villoslada C, Lledo S, et al. Prevalence of pudendal
45 Wrenn K. Fecal impaction. N Engl J Med 1989; 321: 658–62. neuropathy in fecal incontinence: results of a prospective study. Dis
Colon Rectum 1995; 38: 952–58.
46 Donnelly VS, O’Herlihy C, Campbell DM, O’Connell PR.
Postpartum fecal incontinence is more common in women with 69 Gilliland R, Altomare DF, Moreira H Jr, Oliveira L, Gilliland JE,
irritable bowel syndrome. Dis Colon Rectum 1998; 41: 586–89. Wexner SD. Pudendal neuropathy is predictive of failure following
anterior overlapping sphincteroplasty. Dis Colon Rectum 1998; 41:
47 Rockwood TH, Church JM, Fleshman JW, et al. Patient and
1516–22.
surgeon ranking of the severity of symptoms associated with fecal
incontinence: the fecal incontinence severity index. Dis Colon 70 Buie WD, Lowry AC, Rothenberger DA, Madoff RD. Clinical rather
Rectum 1999; 42: 1525–32. than laboratory assessment predicts continence after anterior
sphincteroplasty. Dis Colon Rectum 2001; 44: 1255–60.
48 Engel AF, Kamm MA, Bartram CI, Nicholls RJ. Relationship of
symptoms in faecal incontinence to specific sphincter 71 Hallgren T, Fasth S, Delbro DS, Nordgren S, Oresland T, Hulten L.
abnormalities. Int J Colorectal Dis 1995; 10: 152–55. Loperamide improves anal sphincter function and continence after
restorative proctocolectomy. Dig Dis Sci 1994; 39: 2612–18.
49 Felt-Bersma RJ, Klinkenberg-Knol EC, Meuwissen SG. Anorectal
function investigations in incontinent and continent patients: 72 Donnelly V, O’Connell PR, O’Herlihy C. The influence of oestrogen
differences and discriminatory value. Dis Colon Rectum 1990; 33: replacement on faecal incontinence in postmenopausal women.
479–85. Br J Obstet Gynaecol 1997; 104: 311–15.
630 www.thelancet.com Vol 364 August 14, 2004
For personal use. Only reproduce with permission from Elsevier Ltd
Review
73 Santoro GA, Eitan BZ, Pryde A, Bartolo DC. Open study of low-dose 97 Ryn AK, Morren GL, Hallbook O, Sjodahl R. Long-term results of
amitriptyline in the treatment of patients with idiopathic fecal electromyographic biofeedback training for fecal incontinence.
incontinence. Dis Colon Rectum 2000; 43: 1676–81. Dis Colon Rectum 2000; 43: 1262–66.
74 Kusunoki M, Shoji Y, Ikeuchi H, Yamagata K, Yamamura T, 98 Enck P, Daublin G, Lubke HJ, Strohmeyer G. Long-term efficacy of
Utsunomiya J. Usefulness of valproate sodium for treatment biofeedback training for fecal incontinence. Dis Colon Rectum 1994;
of incontinence after ileoanal anastomosis. Surgery 1990; 107: 37: 997–1001.
311–15. 99 Guillemot F, Bouche B, Gower-Rousseau C, et al. Biofeedback for
75 Carapeti EA, Kamm MA, Evans BK, Phillips RK. Topical the treatment of fecal incontinence. Dis Colon Rectum 1995; 38:
phenylephrine increases anal sphincter resting pressure. Br J Surg 393–97.
1999; 86: 267–70. 100 Nielsen MB, Hauge C, Rasmussen OO, Pedersen JF, Christiansen
76 Carapeti EA, Kamm MA, Nicholls RJ, Phillips RK. Randomized, J. Anal endosonographic findings in the follow-up of primarily
controlled trial of topical phenylephrine for fecal incontinence in sutured sphincteric ruptures. Br J Surg 1992; 79: 104–06.
patients after ileoanal pouch construction. Dis Colon Rectum 2000; 101 Wexner SD, Marchetti F, Jagelman DG. The role of
43: 1059–63. sphincteroplasty for fecal incontinence reevaluated: a prospective
77 Carapeti EA, Kamm MA, Phillips RK. Randomized controlled trial physiologic and functional review. Dis Colon Rectum 1991; 34:
of topical phenylephrine in the treatment of faecal incontinence. 22–30.
Br J Surg 2000; 87: 38–42. 102 Hasegawa H, Yoshioka K, Keighley MR. Randomized trial of
78 Heymen S, Jones KR, Ringel Y, Scarlett Y, Whitehead WE. fecal diversion for sphincter repair. Dis Colon Rectum 2000; 43:
Biofeedback treatment of fecal incontinence: a critical review. 961–64.
Dis Colon Rectum 2001; 44: 728–36. 103 Young CJ, Mathur MN, Eyers AA, Solomon MJ. Successful
79 Wald A. Biofeedback therapy for fecal incontinence. Ann Intern Med overlapping anal sphincter repair: relationship to patient age,
1981; 95: 146–49. neuropathy, and colostomy formation. Dis Colon Rectum 1998;
80 Engel BT, Nikoomanesh P, Schuster MM. Operant conditioning of 41: 344–49.
rectosphincteric responses in the treatment of fecal incontinence. 104 Engel AF, Kamm MA, Sultan AH, Bartram CI, Nicholls RJ.
N Engl J Med 1974; 290: 646–49. Anterior anal sphincter repair in patients with obstetric trauma.
81 Norton C, Kamm MA. Anal sphincter biofeedback and pelvic floor Br J Surg 1994; 81: 1231–34.
exercises for faecal incontinence in adults: a systematic review. 105 Karoui S, Leroi AM, Koning E, Menard JF, Michot F, Denis P.
Aliment Pharmacol Ther 2001; 15: 1147–54. Results of sphincteroplasty in 86 patients with anal incontinence.
82 Fynes MM, Marshall K, Cassidy M, et al. A prospective, randomized Dis Colon Rectum 2000; 43: 813–20.
study comparing the effect of augmented biofeedback with sensory 106 Londono-Schimmer EE, Garcia-Duperly R, Nicholls RJ, Ritchie JK,
biofeedback alone on fecal incontinence after obstetric trauma. Hawley PR, Thomson JP. Overlapping anal sphincter repair for
Dis Colon Rectum 1999; 42: 753–58. faecal incontinence due to sphincter trauma: five year follow-up
83 Goldenberg DA, Hodges K, Hershe T, Jinich H. Biofeedback functional results. Int J Colorectal Dis 1994; 9: 110–13.
therapy for fecal incontinence. Am J Gastroenterol 1980; 74: 107 Halverson AL, Hull TL. Long-term outcome of overlapping anal
342–45. sphincter repair. Dis Colon Rectum 2002; 45: 345–48.
84 Latimer PR, Campbell D, Kasperski J. A components analysis of 108 Malouf AJ, Norton CS, Engel AF, Nicholls RJ, Kamm MA. Long-
biofeedback in the treatment of fecal incontinence. term results of overlapping anterior anal-sphincter repair for
Biofeedback Self Regul 1984; 9: 311–24. obstetric trauma. Lancet 2000; 355: 260–65.
85 Miner PB, Donnelly TC, Read NW. Investigation of mode of action 109 Rothbarth J, Bemelman WA, Meijerink WJ,
of biofeedback in treatment of fecal incontinence. Dig Dis Sci 1990; Buyze-Westerweel ME, van Dijk JG, Delemarre JB. Long-term
35: 1291–98. results of anterior anal sphincter repair for fecal incontinence due
86 Constantinides CG, Cywes S. Fecal incontinence: a simple to obstetric injury. Dig Surg 2000; 17: 390–93.
pneumatic device for home biofeedback training. J Pediatr Surg 110 Sangwan YP, Coller JA, Barrett RC, et al. Unilateral pudendal
1983; 18: 276–77. neuropathy: impact on outcome of anal sphincter repair. Dis Colon
87 Solomon MJ, Pager CK, Rex J, Roberts R, Manning J. Randomized, Rectum 1996; 39: 686–89.
controlled trial of biofeedback with anal manometry, transanal 111 Pinedo G, Vaizey CJ, Nicholls RJ, Roach R, Halligan S, Kamm MA.
ultrasound, or pelvic floor retraining with digital guidance alone in Results of repeat anal sphincter repair. Br J Surg 1999; 86: 66–69.
the treatment of mild to moderate fecal incontinence. Dis Colon 112 Giordano P, Renzi A, Efron J, et al. Previous sphincter repair does
Rectum 2003; 46: 703–10. not affect the outcome of repeat repair. Dis Colon Rectum 2002; 45:
88 Whitehead WE, Burgio KL, Engel BT. Biofeedback treatment of 635–40.
fecal incontinence in geriatric patients. J Am Geriatr Soc 1985; 33: 113 Devesa JM, Vicente E, Enriquez JM, et al. Total fecal
320–24. incontinence–a new method of gluteus maximus transposition:
89 McHugh S, Walma K, Diamant NE. Fecal incontinence: a preliminary results and report of previous experience with similar
controlled trial of biofeedback. Gastroenterology 1986; 90: 154–55. procedures. Dis Colon Rectum 1992; 35: 339–49.
90 Norton C, Kamm MA. Outcome of biofeedback for faecal 114 Konsten J, Baeten CGMI, Havenith MG, Soeters PB. Morphology
incontinence. Br J Surg 1999; 86: 1159–63. of dynamic graciloplasty compared with the anal sphincter.
91 Jensen LL, Lowry AC. Biofeedback improves functional outcome Dis Colon Rectum 1993; 36: 559–63.
after sphincteroplasty. Dis Colon Rectum 1997; 40: 197–200. 115 Baeten C, Spaans F, Fluks A. An implanted neuromuscular
92 Rieger NA, Wattchow DA, Sarre RG, et al. Prospective trial of pelvic stimulator for fecal continence following previously implanted
floor retraining in patients with fecal incontinence. Dis Colon gracilis muscle: report of a case. Dis Colon Rectum 1988; 31:
Rectum 1997; 40: 821–26. 134–37.
93 van Tets WF, Kuijpers JH, Bleijenberg G. Biofeedback treatment is 116 Madoff RD, Rosen HR, Baeten CG, et al. Safety and efficacy
ineffective in neurogenic fecal incontinence. Dis Colon Rectum of dynamic muscle plasty for anal incontinence: lessons from a
1996; 39: 992–94. prospective, multicenter trial. Gastroenterology 1999; 116: 549–56.
94 Norton C, Hosker G, Brazzelli M. Biofeedback and/or sphincter 117 Baeten CG, Bailey HR, Bakka A, et al. Safety and efficacy of
exercises for the treatment of faecal incontinence in adults. dynamic graciloplasty for fecal incontinence: report of a prospective,
Cochrane Database Syst Rev 2000: CD002111. multicenter trial. Dis Colon Rectum 2000; 43: 743–51.
95 Loening-Baucke V. Efficacy of biofeedback training in improving 118 Christiansen J, Lorentzen M. Implantation of artificial sphincter for
faecal incontinence and anorectal physiologic function. Gut 1990; anal incontinence. Lancet 1987; 2: 244–45.
31: 1395–402. 119 Altomare DF, Dodi G, La Torre F, Romano G, Melega E, Rinaldi M.
96 Norton C, Chelvanayagam S, Wilson-Barnett J, Redfern S, Multicentre retrospective analysis of the outcome of artificial anal
Kamm MA. Randomized controlled trial of biofeedback for fecal sphincter implantation for severe faecal incontinence. Br J Surg
incontinence. Gastroenterology 2003; 125: 1320–29. 2001; 88: 1481–86.
www.thelancet.com Vol 364 August 14, 2004 631
For personal use. Only reproduce with permission from Elsevier Ltd
Review
120 O’Brien PE, Skinner S. Restoring control: the Acticon Neosphincter 132 Matzel KE, Kamm ME, Stosser M, et al. Sacral spine nerve
artificial bowel sphincter in the treatment of anal incontinence. stimulation for faecal incontinence: multicentre study. Lancet
Dis Colon Rectum 2000; 43: 1213–16. 2004; 363: 1270–76.
121 Christiansen J, Rasmussen OO, Lindorff-Larsen K. Long-term 133 Rosen HR, Urbarz C, Holzer B, Novi G, Schiessel R. Sacral nerve
results of artificial anal sphincter implantation for severe anal stimulation as a treatment for fecal incontinence. Gastroenterology
incontinence. Ann Surg 1999; 230: 45–48. 2001; 121: 536–41.
122 Wong WD, Jensen LL, Bartolo DC, Rothenberger DA. Artificial anal 134 Feretis C, Benakis P, Dailianas A, et al. Implantation of
sphincter. Dis Colon Rectum 1996; 39: 1345–51. microballoons in the management of fecal incontinence.
123 Lehur PA, Roig JV, Duinslaeger M. Artificial anal sphincter: Dis Colon Rectum 2001; 44: 1605–09.
prospective clinical and manometric evaluation. Dis Colon Rectum 135 Weiss E, Efron J, Nogueras J, Wexner S. Submucosal injection of
2000; 43: 1100–06. carbon-coated beads is a successful and safe office-based
124 Malouf AJ, Vaizey CJ, Kamm MA, Nicholls RJ. Reassessing artificial treatment of fecal incontinence. Dis Colon Rectum 2002; 45:
bowel sphincters. Lancet 2000; 355: 2219–20. A46–47 (abstr).
125 Wong WD, Congliosi SM, Spencer MP, et al. The safety and efficacy 136 Shafik A. Perianal injection of autologous fat for treatment
of the artificial bowel sphincter for fecal incontinence: results from of sphincteric incontinence. Dis Colon Rectum 1995; 38:
a multicenter cohort study. Dis Colon Rectum 2002; 45: 1139–53. 583–87.
126 Matzel KE, Stadelmaier U, Hohenfellner M, Gall FP. Electrical 137 Malouf AJ, Vaizey CJ, Norton CS, Kamm MA. Internal anal
stimulation of sacral spinal nerves for treatment of faecal sphincter augmentation for fecal incontinence using injectable
incontinence. Lancet 1995; 346: 1124–7. silicone biomaterial. Dis Colon Rectum 2001; 44: 595–600.
127 Matzel KE, Stadelmaier U, Hohenfellner M, Hohenberger W. 138 Kumar D, Benson MJ, Bland JE. Glutaraldehyde cross-linked
Chronic sacral spinal nerve stimulation for fecal incontinence: long- collagen in the treatment of faecal incontinence. Br J Surg 1998;
term results with foramen and cuff electrodes. Dis Colon Rectum 85: 978–79.
2001; 44: 59–66. 139 Kenefick NJ, Vaizey CJ, Malouf AJ, Norton CS, Marshall M,
128 Matzel KE, Kamm MA, Stosser M, et al. Sacral spinal nerve Kamm MA. Injectable silicone biomaterial for faecal incontinence
stimulation for faecal incontinence: multicentre study. Lancet 2004; due to internal anal sphincter dysfunction. Gut 2002; 51:
363: 1270–76. 225–28.
129 Vaizey CJ, Kamm MA, Turner IC, Nicholls RJ, Woloszko J. Effects 140 Takahashi T, Garcia-Osogobio S, Valdovinos MA, Belmonte C,
of short term sacral nerve stimulation on anal and rectal function in Barreto C, Velasco L. Extended two-year results of radio-frequency
patients with anal incontinence. Gut 1999; 44: 407–12. energy delivery for the treatment of fecal incontinence (the Secca
130 Malouf AJ, Vaizey CJ, Nicholls RJ, Kamm MA. Permanent sacral procedure). Dis Colon Rectum 2003; 46: 711–15.
nerve stimulation for fecal incontinence. Ann Surg 2000; 232: 141 Efron J, Corman ML, Fleshman J, et al. Safety and effectiveness
143–48. of temperature-controlled radio-frequency energy delivered to
131 Ganio E, Ratto C, Masin A, et al. Neuromodulation for fecal the anal canal (Secca procedure) for the treatment of fecal
incontinence: outcome in 16 patients with definitive implant: the incontinence. Dis Colon Rectum 2003; 46: 1606–16.
initial Italian Sacral Neurostimulation Group (GINS) experience.
Dis Colon Rectum 2001; 44: 965–70.
632 www.thelancet.com Vol 364 August 14, 2004
For personal use. Only reproduce with permission from Elsevier Ltd
Anda mungkin juga menyukai
- B3 - Sample Cases of PlagiarismDokumen6 halamanB3 - Sample Cases of PlagiarismJoana Marie CruzBelum ada peringkat
- The Chick Brain in Stereotaxic Coordinates and Alternate Stains: Featuring Neuromeric Divisions and Mammalian HomologiesDari EverandThe Chick Brain in Stereotaxic Coordinates and Alternate Stains: Featuring Neuromeric Divisions and Mammalian HomologiesBelum ada peringkat
- VCE Biology Unit 3 Summaries - Immune SystemDokumen7 halamanVCE Biology Unit 3 Summaries - Immune SystemDJTofiBelum ada peringkat
- ClinicalsignificanceB PDFDokumen14 halamanClinicalsignificanceB PDFLiliann RiveraBelum ada peringkat
- Neurohormonal Regulation of Body FunctionsDokumen34 halamanNeurohormonal Regulation of Body FunctionsjimmyBelum ada peringkat
- Reproducing The Wechsler Intelligence Scale For Children-Fifth Edition: Factor Model ResultsDokumen5 halamanReproducing The Wechsler Intelligence Scale For Children-Fifth Edition: Factor Model ResultsRISKI DAMAYBelum ada peringkat
- A Brief History of The Origins of Behavioral MedicineDokumen16 halamanA Brief History of The Origins of Behavioral MedicineAllie WatrenBelum ada peringkat
- Group Medical Appointments: An Introduction for Health ProfessionalsDari EverandGroup Medical Appointments: An Introduction for Health ProfessionalsPenilaian: 5 dari 5 bintang5/5 (1)
- Fiqh Us Sunnah Complete by Sayyid SabiqDokumen451 halamanFiqh Us Sunnah Complete by Sayyid SabiqUmm Eris Arleta AmatullahBelum ada peringkat
- Dietician Referral Ms SmithDokumen3 halamanDietician Referral Ms SmithPrasoon Premraj0% (1)
- Nursing Pharmacology Sample Exam QuestionsDokumen3 halamanNursing Pharmacology Sample Exam QuestionsDhreambhig Ahrchorphul100% (1)
- (Mark S. Schwartz PHD, Frank Andrasik PHD) BiofeedDokumen933 halaman(Mark S. Schwartz PHD, Frank Andrasik PHD) BiofeedÁngela María Páez BuitragoBelum ada peringkat
- EnuresisDokumen11 halamanEnuresisadrianaBelum ada peringkat
- Hara Issue 1Dokumen110 halamanHara Issue 1NaturelandBelum ada peringkat
- SchizophreniaDokumen9 halamanSchizophreniavinodksahuBelum ada peringkat
- Frontal Lobe Syndromes: BackgroundDokumen2 halamanFrontal Lobe Syndromes: BackgroundFausiah Ulva MBelum ada peringkat
- Brain Fitness For Positive AgingDokumen65 halamanBrain Fitness For Positive AgingMary GomezBelum ada peringkat
- Six Super Skills For Executive FunctioningDokumen178 halamanSix Super Skills For Executive Functioningsupervisão ABA construirBelum ada peringkat
- Syllabus Psychiatry Clerkship 2018 19Dokumen8 halamanSyllabus Psychiatry Clerkship 2018 19Tyler KingBelum ada peringkat
- PNES ClinicalApproachesDokumen19 halamanPNES ClinicalApproachesClaudiaBelum ada peringkat
- Cognitive Rehabilitation in Acquired Brain Injury: Srikant V Moderator: DR Nidhi RawatDokumen64 halamanCognitive Rehabilitation in Acquired Brain Injury: Srikant V Moderator: DR Nidhi RawatpustuleBelum ada peringkat
- Chapter 3-1-15Dokumen11 halamanChapter 3-1-15Winda AnnishaBelum ada peringkat
- 09 Central Nervous System Coloring BookDokumen11 halaman09 Central Nervous System Coloring BookArmy JmBelum ada peringkat
- PHYSIOTIMES Vol.7, Issue 5, March'2016Dokumen1 halamanPHYSIOTIMES Vol.7, Issue 5, March'2016PHYSIOTIMESBelum ada peringkat
- Applying Modern Pain Neuroscience in Clinical - 2014Dokumen12 halamanApplying Modern Pain Neuroscience in Clinical - 2014Juci FreitasBelum ada peringkat
- Schizotipy Review and Relationship With SchizophreniaDokumen11 halamanSchizotipy Review and Relationship With Schizophreniasofian2pBelum ada peringkat
- Fish Psychopathology Book ReviewDokumen2 halamanFish Psychopathology Book ReviewAbhishek Sāmal0% (1)
- Cognitive Function in Schizophrenia A Review 187 PDFDokumen8 halamanCognitive Function in Schizophrenia A Review 187 PDFEvaBelum ada peringkat
- Localization NeurofeedbackDokumen16 halamanLocalization NeurofeedbackKashyapi thakuriaBelum ada peringkat
- Reading Test - SchizophreniaDokumen9 halamanReading Test - SchizophreniaOlive GroupBelum ada peringkat
- Brain, Vision, Memory - Charles G. Gross PDFDokumen262 halamanBrain, Vision, Memory - Charles G. Gross PDFDumi AlexBelum ada peringkat
- Leading-Edge NeuroscienceDokumen3 halamanLeading-Edge Neurosciencegabyk68Belum ada peringkat
- Neurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoDokumen43 halamanNeurobiology of Anxiety Disorders: Michael J. Meaney, Michael R. Liebowitz, and E. David LeonardoOscar René Hernández PérezBelum ada peringkat
- Suppl55 PDFDokumen310 halamanSuppl55 PDFUbaidillah Romadlon AlfairuziBelum ada peringkat
- (Therapy in Practice Series 30) James Law (Auth.), James Law BA, MCSLT (Eds.) - The Early Identification of Language Impairment in Children-Springer US (1992)Dokumen212 halaman(Therapy in Practice Series 30) James Law (Auth.), James Law BA, MCSLT (Eds.) - The Early Identification of Language Impairment in Children-Springer US (1992)Catalina CristoiuBelum ada peringkat
- MHA Ect GuidelinesDokumen151 halamanMHA Ect GuidelinesDian AfrisiaBelum ada peringkat
- Stress Management Techniques Evidencebased Procedures That Reduce Stress and Promote Health PDFDokumen16 halamanStress Management Techniques Evidencebased Procedures That Reduce Stress and Promote Health PDFMaica MagbitangBelum ada peringkat
- The Neurosequential Network: Janelle Rose, L.M.F.TDokumen1 halamanThe Neurosequential Network: Janelle Rose, L.M.F.Tapi-553045669Belum ada peringkat
- Pharmaco Vigilance of ASU Drugs:an Over View of Current Status, Challenges and SolutionsDokumen55 halamanPharmaco Vigilance of ASU Drugs:an Over View of Current Status, Challenges and Solutionssuhas M100% (1)
- Burnout-Depression Overlap - A ReviewDokumen15 halamanBurnout-Depression Overlap - A ReviewMarcelo PinheiroBelum ada peringkat
- StatusEpilepticus Pocket CardDokumen2 halamanStatusEpilepticus Pocket CardDiana MihaiBelum ada peringkat
- Conners2011 PDFDokumen297 halamanConners2011 PDFCristinaBelum ada peringkat
- JACOBSON & GREENLEY - What Is Recovery A Conceptual Model and ExplicationDokumen4 halamanJACOBSON & GREENLEY - What Is Recovery A Conceptual Model and ExplicationemaildegeorgeBelum ada peringkat
- Self Cingulo PosteriorDokumen7 halamanSelf Cingulo PosteriorJose ZapataBelum ada peringkat
- Clinical Problems Associated With Aging ProcessDokumen28 halamanClinical Problems Associated With Aging Processهنادي رازمBelum ada peringkat
- Framework For Professional PracticeDokumen26 halamanFramework For Professional PracticeAdvait GulatiBelum ada peringkat
- 1994 - Functional Psychiatric Disorders of The Elderly - Chiu & AmesDokumen652 halaman1994 - Functional Psychiatric Disorders of The Elderly - Chiu & AmesCarlos LengemannBelum ada peringkat
- Guidline Threatment For of Alcohol Use DisorderDokumen226 halamanGuidline Threatment For of Alcohol Use Disorderafifberlian100% (1)
- Guideline LVM - EscarasDokumen94 halamanGuideline LVM - EscarasCarla SantosBelum ada peringkat
- EEG MaturationDokumen29 halamanEEG Maturationhm3398Belum ada peringkat
- Biological Basis of BehaviorDokumen8 halamanBiological Basis of BehaviorLaine DerainBelum ada peringkat
- Vernon MouncastleDokumen40 halamanVernon MouncastleCarla Guixé SendiuBelum ada peringkat
- Guidance For CBRTDokumen153 halamanGuidance For CBRTkbl27Belum ada peringkat
- Neuroimaging Biomarkers in Alzheimer's DiseaseDokumen136 halamanNeuroimaging Biomarkers in Alzheimer's DiseaseInternational Medical PublisherBelum ada peringkat
- A Clinical Casebook: Fundamentals of Diagnosing and Treating Eating DisordersDokumen159 halamanA Clinical Casebook: Fundamentals of Diagnosing and Treating Eating DisordersDaoud IssaBelum ada peringkat
- Mu Rythm in Children and SymptomsDokumen94 halamanMu Rythm in Children and SymptomsAdrian GtBelum ada peringkat
- The Use of Mobile Device Application For Assessing Pain Pattern in Veteran Patients With Mild Traumatic Brain Injury Related HeadachesDokumen27 halamanThe Use of Mobile Device Application For Assessing Pain Pattern in Veteran Patients With Mild Traumatic Brain Injury Related Headachesapi-529388510Belum ada peringkat
- Complications of Ischemic StrokeDokumen40 halamanComplications of Ischemic StrokeVitas HaryantoBelum ada peringkat
- Educational Material: Educational Skills Workshop 25, 27 Hands-On PolysomnographyDokumen136 halamanEducational Material: Educational Skills Workshop 25, 27 Hands-On PolysomnographyPhạm Văn HiệpBelum ada peringkat
- Ylvisaker, Turkstra, Coelho Beh & Soc TX Sem 2005 PDFDokumen12 halamanYlvisaker, Turkstra, Coelho Beh & Soc TX Sem 2005 PDFmichelle montesBelum ada peringkat
- Chronic Pain Clinical Updates and PerspectivesDokumen248 halamanChronic Pain Clinical Updates and PerspectivesAlonso CastañoBelum ada peringkat
- ACT For Psychosis Workshop BABCP 2008 Eric Morris Gordon Mitchell Amy McArthurDokumen11 halamanACT For Psychosis Workshop BABCP 2008 Eric Morris Gordon Mitchell Amy McArthurjlbermudezc100% (1)
- Psychiatric Diagnosis: Challenges and ProspectsDari EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumPenilaian: 5 dari 5 bintang5/5 (1)
- Approach To The Adult Patient With Fever of Unknown OriginDokumen6 halamanApproach To The Adult Patient With Fever of Unknown Origini can always make u smile :D100% (1)
- Irritable Bowel SyndromeDokumen2 halamanIrritable Bowel Syndromei can always make u smile :DBelum ada peringkat
- Locomotor ExamDokumen6 halamanLocomotor Exami can always make u smile :D100% (1)
- Cardiovascular Disease in Women: Quality in Practice CommitteeDokumen24 halamanCardiovascular Disease in Women: Quality in Practice Committeei can always make u smile :DBelum ada peringkat
- Investigations in Rheumatology: What's New?Dokumen10 halamanInvestigations in Rheumatology: What's New?i can always make u smile :DBelum ada peringkat
- Fob ExplainDokumen1 halamanFob Explaini can always make u smile :DBelum ada peringkat
- Genetics and Bowel CancerDokumen5 halamanGenetics and Bowel Canceri can always make u smile :DBelum ada peringkat
- NEUROANATOMY MCQ's Summer 2004Dokumen2 halamanNEUROANATOMY MCQ's Summer 2004i can always make u smile :DBelum ada peringkat
- Neuroanatomy MCQDokumen7 halamanNeuroanatomy MCQi can always make u smile :D78% (9)
- Transf PT InfoDokumen6 halamanTransf PT Infoi can always make u smile :DBelum ada peringkat
- Diagnostic Handbook of OtorhinolaryngologyDokumen271 halamanDiagnostic Handbook of Otorhinolaryngologyi can always make u smile :D100% (2)
- Measuring Fecal IncontinenceDokumen15 halamanMeasuring Fecal Incontinencei can always make u smile :D100% (1)
- The Fecal Incontinence Severity IndexDokumen7 halamanThe Fecal Incontinence Severity Indexi can always make u smile :DBelum ada peringkat
- Nationaln Tle: National Audit of Continence Care: Laying The FoundationDokumen23 halamanNationaln Tle: National Audit of Continence Care: Laying The Foundationi can always make u smile :DBelum ada peringkat
- Continence AuditDokumen6 halamanContinence Auditi can always make u smile :DBelum ada peringkat
- Intrapartum HandoutDokumen29 halamanIntrapartum HandoutZahBelum ada peringkat
- SWAN Parkinson MRIDokumen9 halamanSWAN Parkinson MRIulfi yunitaBelum ada peringkat
- First Aid For The Usmle Step 1 2022-Mcgraw-Hill Education 2022Dokumen1 halamanFirst Aid For The Usmle Step 1 2022-Mcgraw-Hill Education 2022Beto RendonBelum ada peringkat
- Ayur TabletDokumen11 halamanAyur TabletNarasannapeta PatanjaliBelum ada peringkat
- Lange Gynecology MCQ 2Dokumen5 halamanLange Gynecology MCQ 2BassamSheryan0% (1)
- Common Pediatric DiseasesDokumen16 halamanCommon Pediatric Diseasesboxed juiceBelum ada peringkat
- Hepatology Research - 2023 - Yoshiji - Management of Cirrhotic Ascites Seven Step Treatment Protocol Based On The JapaneseDokumen12 halamanHepatology Research - 2023 - Yoshiji - Management of Cirrhotic Ascites Seven Step Treatment Protocol Based On The JapaneseSarah FaziraBelum ada peringkat
- Hemotology ReviewDokumen61 halamanHemotology ReviewSukma EffendyBelum ada peringkat
- The Pediatric Physical Exam:: Who, When, What and Why?Dokumen26 halamanThe Pediatric Physical Exam:: Who, When, What and Why?Carlo Emmanuel SantosBelum ada peringkat
- Effects of Advanced Carbohydrate Counting On Glucose Control and QolDokumen9 halamanEffects of Advanced Carbohydrate Counting On Glucose Control and QollloplBelum ada peringkat
- Health Grade10 4th QuarterDokumen40 halamanHealth Grade10 4th QuarterYnjel HilarioBelum ada peringkat
- I. General Physical AssessmentDokumen5 halamanI. General Physical AssessmentmnlstrBelum ada peringkat
- EMPANELEDHOSPITALLISTDokumen12 halamanEMPANELEDHOSPITALLISTVsknBelum ada peringkat
- DR Cowan On Mask StudyDokumen3 halamanDR Cowan On Mask StudyK Mehmet ŞensoyBelum ada peringkat
- TURBT FinalDokumen52 halamanTURBT FinalMuhammad RafiBelum ada peringkat
- Cost Per Test PC400 2020Dokumen10 halamanCost Per Test PC400 2020fischaBelum ada peringkat
- PPT-"Services and Benefits For Gulf War Veterans" - Anthony HardieDokumen98 halamanPPT-"Services and Benefits For Gulf War Veterans" - Anthony HardieAnthony Hardie100% (5)
- Summer PromoDokumen1 halamanSummer PromobarilesBelum ada peringkat
- Slide Materi Dr. Kevin Triangto, SPKFR - Heart Failure - PMR4GP 2022Dokumen27 halamanSlide Materi Dr. Kevin Triangto, SPKFR - Heart Failure - PMR4GP 2022Maulia Wisda Era ChresiaBelum ada peringkat
- Research Revision Version 10 (Clean Copy)Dokumen27 halamanResearch Revision Version 10 (Clean Copy)Nesty Perez IIIBelum ada peringkat
- Ouabain - The Optimal Solution For The Problem of Myocardial InfarctionDokumen20 halamanOuabain - The Optimal Solution For The Problem of Myocardial InfarctionredsbooksBelum ada peringkat
- Sugar and Blood 2Dokumen19 halamanSugar and Blood 2shaira ubaldeBelum ada peringkat
- Isolation and Identification of Avibacterium Paragallinarum From Layer Chickens in Gazipur, BangladeshDokumen3 halamanIsolation and Identification of Avibacterium Paragallinarum From Layer Chickens in Gazipur, BangladeshMd. Ehsanul Haque100% (1)
- Malunggay Leaf ResearchDokumen3 halamanMalunggay Leaf ResearchEj KasimBelum ada peringkat
- Final Diabetes & Its Role in PeriodonticsDokumen140 halamanFinal Diabetes & Its Role in Periodonticsvinay jainBelum ada peringkat
- Child Guidance ClinicDokumen22 halamanChild Guidance ClinicBinal Joshi67% (3)
- ICU One Pager NIPPVDokumen1 halamanICU One Pager NIPPVNicholas HelmstetterBelum ada peringkat