Anda mungkin juga menyukai
- Menopause Concept MapDokumen1 halamanMenopause Concept MapBritanny NelsonBelum ada peringkat
- USMLE 1 Hematology BookDokumen368 halamanUSMLE 1 Hematology BookPRINCEBelum ada peringkat
- Answer: CDokumen34 halamanAnswer: CLola OladapoBelum ada peringkat
- Untitled DocumentDokumen6 halamanUntitled Documentانس ابوهيبةBelum ada peringkat
- This Study Resource Was: Hesi Pharmacology Test Bank 2018 RN V2 14 Total QuestionsDokumen3 halamanThis Study Resource Was: Hesi Pharmacology Test Bank 2018 RN V2 14 Total QuestionsCrystal B Costa78Belum ada peringkat
- AntidotesDokumen2 halamanAntidotesYemaya84Belum ada peringkat
- Pharmacology test tasks on cardiac glycosides and antiarrhythmic drugsDokumen19 halamanPharmacology test tasks on cardiac glycosides and antiarrhythmic drugsBlessing NwosuBelum ada peringkat
- Atrial Fibrillation and Dysrhythmias GuideDokumen10 halamanAtrial Fibrillation and Dysrhythmias Guideyaneidys perezBelum ada peringkat
- Nclex RN Sata CompilationDokumen10 halamanNclex RN Sata CompilationJanna mae PatriarcaBelum ada peringkat
- Concept Map Et Al 11-04-15Dokumen7 halamanConcept Map Et Al 11-04-15api-353656227Belum ada peringkat
- AdultDokumen295 halamanAdultKen WonBelum ada peringkat
- 5 Types of QuestionsDokumen5 halaman5 Types of QuestionsQwequ Gong AnanseBelum ada peringkat
- Hyperemesis Gravidarum: Bleeding Complications of PregnancyDokumen6 halamanHyperemesis Gravidarum: Bleeding Complications of PregnancykirbsBelum ada peringkat
- U World Endocrine FinalDokumen12 halamanU World Endocrine Finalsean blazeBelum ada peringkat
- Newborn Care 1Dokumen6 halamanNewborn Care 1Francine LaxaBelum ada peringkat
- Medsurge RationaleDokumen8 halamanMedsurge RationaleRose Anne AbivaBelum ada peringkat
- Jennifer Portillo Health Assessment VocabularyDokumen9 halamanJennifer Portillo Health Assessment VocabularyJennifer PortilloBelum ada peringkat
- Flashcards for Admin ConsiderationsDokumen1 halamanFlashcards for Admin ConsiderationsAntonette Joy SolinapBelum ada peringkat
- Nursing Cram Sheet For The NCLEX-RN: TestinformationDokumen7 halamanNursing Cram Sheet For The NCLEX-RN: Testinformationjanns tumanengBelum ada peringkat
- Test-Taking Tips For NCLEXDokumen59 halamanTest-Taking Tips For NCLEXJbl2328Belum ada peringkat
- Review of Systems ANDREADokumen7 halamanReview of Systems ANDREAAndrea Dora OrtalizBelum ada peringkat
- Insulin ChartDokumen1 halamanInsulin ChartChristian BagaresBelum ada peringkat
- UntitledDokumen41 halamanUntitledvioletdeocaresBelum ada peringkat
- NCLEX 2007 BulletinDokumen44 halamanNCLEX 2007 Bulletinij22comBelum ada peringkat
- Don't Delegate What You Can Evaluate, Assess, TeachDokumen35 halamanDon't Delegate What You Can Evaluate, Assess, TeachZOEYVALBelum ada peringkat
- NCLEX Study MaterialDokumen40 halamanNCLEX Study MaterialChristie GerconBelum ada peringkat
- Stages of ShockDokumen7 halamanStages of ShockNicholas TagleBelum ada peringkat
- Endocrine System Study Guide: Hormones & GlandsDokumen5 halamanEndocrine System Study Guide: Hormones & GlandsClaudia SanchezBelum ada peringkat
- TonsillitisDokumen1 halamanTonsillitisVishalBelum ada peringkat
- Pharm WorksheetsDokumen29 halamanPharm Worksheetsj.siemens1dBelum ada peringkat
- Ati QuestionsDokumen2 halamanAti Questionsnjames44Belum ada peringkat
- Nursing BulletsDokumen72 halamanNursing BulletsJoanna Mae Carolino100% (1)
- Quizlet (2) RRRRRDokumen7 halamanQuizlet (2) RRRRRGina GiammalvoBelum ada peringkat
- EndocrineDokumen2 halamanEndocrineUnclePorkchopBelum ada peringkat
- Invega+Sustenna PiDokumen18 halamanInvega+Sustenna PiMaal AbrarBelum ada peringkat
- Table of Sedative, Hypnotic, AntianxietyDokumen4 halamanTable of Sedative, Hypnotic, AntianxietyirfanzukriBelum ada peringkat
- Acid and Base Balance and ImbalanceDokumen38 halamanAcid and Base Balance and ImbalanceMustafa KhandgawiBelum ada peringkat
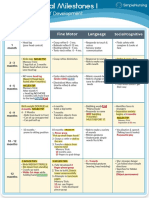
- Visual Chart 1 - Developmental MilestonesDokumen1 halamanVisual Chart 1 - Developmental MilestonesVishalBelum ada peringkat
- Nursing BulletsDokumen83 halamanNursing BulletsgilissaBelum ada peringkat
- Pharmacology Exam4 ReviewDokumen8 halamanPharmacology Exam4 ReviewNatalia BortellBelum ada peringkat
- GambarDokumen27 halamanGambarAnonymous feLB4alTBelum ada peringkat
- NursingDokumen8 halamanNursingWen SilverBelum ada peringkat
- NCLEX Review NotesDokumen20 halamanNCLEX Review Notesshaali86Belum ada peringkat
- 35 Nclex QuestionsDokumen6 halaman35 Nclex Questionsjohnnymyunghee0% (1)
- Respiratory Pneumonia PathophysiologyDokumen1 halamanRespiratory Pneumonia PathophysiologyTrisha VergaraBelum ada peringkat
- ABCDE Approach to Assessing and Treating the Acutely Ill PatientDokumen22 halamanABCDE Approach to Assessing and Treating the Acutely Ill PatientSarah RamliBelum ada peringkat
- Immunity 1Dokumen6 halamanImmunity 1Tori RolandBelum ada peringkat
- Oncology - Cancer PreventionDokumen1 halamanOncology - Cancer PreventionElla MejiaBelum ada peringkat
- DIABETES MELLITUS PATHOPHYSIOLOGY, TYPES, AND MANAGEMENTDokumen66 halamanDIABETES MELLITUS PATHOPHYSIOLOGY, TYPES, AND MANAGEMENTElvis J. DavisBelum ada peringkat
- Neuro, GI, GU, MSK midterm and final reviewDokumen3 halamanNeuro, GI, GU, MSK midterm and final reviewjenn1722Belum ada peringkat
- Lippincott's REPRODUCTIVE PROBLEMSDokumen14 halamanLippincott's REPRODUCTIVE PROBLEMSNursyNurseBelum ada peringkat
- C. Nursing Interventions - D. Prevention of ComplicationsDokumen5 halamanC. Nursing Interventions - D. Prevention of ComplicationsbaconhaterBelum ada peringkat
- Terminology of PsychiatryDokumen6 halamanTerminology of PsychiatryHassan.shehri100% (1)
- Alcohol Withdrawal and Dementia Safety TeachingDokumen2 halamanAlcohol Withdrawal and Dementia Safety TeachingestberryBelum ada peringkat
- Prof. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesDokumen5 halamanProf. Sandra M. Covarrubias - September 24, 2021: 5.2fluid & Electrolytes ImbalancesIvy VillalobosBelum ada peringkat
- Nclex Tips - September 25, 2007Dokumen19 halamanNclex Tips - September 25, 2007male nurseBelum ada peringkat
- Parenting Styles: - Dictatorial or AuthoritarianDokumen45 halamanParenting Styles: - Dictatorial or AuthoritarianCourseTree LearningBelum ada peringkat
- A-T-I Endocrine NotesDokumen3 halamanA-T-I Endocrine NotesKelseyAnnBarnesBelum ada peringkat
- Drug Card Solu-MEDROLDokumen2 halamanDrug Card Solu-MEDROLBenBelum ada peringkat
- Medsurg PrintDokumen82 halamanMedsurg PrintjennywatsurproblemBelum ada peringkat
- Communicable DiseasesDokumen50 halamanCommunicable Diseasesitsme_riza100% (2)
- EPI Nursing ConsiderationsDokumen2 halamanEPI Nursing ConsiderationsBel Allen83% (6)
- Respiratory SystemDokumen14 halamanRespiratory Systemitsme_rizaBelum ada peringkat
- Drains ReviewerDokumen2 halamanDrains Revieweritsme_rizaBelum ada peringkat
- Gastrointestinal SystemDokumen44 halamanGastrointestinal Systemitsme_rizaBelum ada peringkat
- Perioperative NursingDokumen5 halamanPerioperative Nursingitsme_rizaBelum ada peringkat
- Drains ReviewerDokumen2 halamanDrains Revieweritsme_rizaBelum ada peringkat
- READ: Psalm 103: 1-10: "Adding Up Your Blessing Will Multiply Your Joy."Dokumen1 halamanREAD: Psalm 103: 1-10: "Adding Up Your Blessing Will Multiply Your Joy."itsme_rizaBelum ada peringkat
- Hematologic SystemDokumen32 halamanHematologic Systemitsme_rizaBelum ada peringkat
- Alcohol Screening TestDokumen3 halamanAlcohol Screening Testitsme_rizaBelum ada peringkat
- PDF Sunset and Desire by Paz LatorenaDokumen12 halamanPDF Sunset and Desire by Paz LatorenaBebelyn PatricioBelum ada peringkat
- Assessment of Fluid and ElectrolyteDokumen15 halamanAssessment of Fluid and ElectrolyteDip Ayan MBelum ada peringkat
- Autonomic Nervous System For MBBSDokumen20 halamanAutonomic Nervous System For MBBSjacobsBelum ada peringkat
- PhotosynthesisDokumen6 halamanPhotosynthesisFuturephd3000Belum ada peringkat
- Fever PathophysiologyDokumen9 halamanFever PathophysiologyNadya AzzahraBelum ada peringkat
- Qualitative Tests for Bile ComponentsDokumen8 halamanQualitative Tests for Bile ComponentsSoh Rodriguez100% (1)
- Analysis - Bio - NEET 2023Dokumen5 halamanAnalysis - Bio - NEET 2023oniichanBelum ada peringkat
- Hoa Silver Edition Manual V1 5-0-120308 enDokumen23 halamanHoa Silver Edition Manual V1 5-0-120308 enAlex KrobbachBelum ada peringkat
- BIO01 CO1 PPT - An Overview of The CellDokumen60 halamanBIO01 CO1 PPT - An Overview of The CellCHRISTIAN MATTHEW DELA CRUZBelum ada peringkat
- 11.transportation in Plants & AnimalsDokumen51 halaman11.transportation in Plants & AnimalsReshma ModhiaBelum ada peringkat
- Blueprint of LifeDokumen42 halamanBlueprint of Lifesophiehee1234Belum ada peringkat
- Ayurveda Physical BodyDokumen11 halamanAyurveda Physical BodyanantBelum ada peringkat
- Lefort 1 OsteotomyDokumen16 halamanLefort 1 Osteotomyabhiram.ramesh1290Belum ada peringkat
- Simple Non-Ruminants: Principles of Animal Nutrition Dr. Cristine W. MaramagDokumen30 halamanSimple Non-Ruminants: Principles of Animal Nutrition Dr. Cristine W. MaramagMc Kjell Dagman RaveloBelum ada peringkat
- Vocal AnatomyDokumen8 halamanVocal AnatomyfunktotumBelum ada peringkat
- Anatomy & Physiology of DengueDokumen8 halamanAnatomy & Physiology of DengueYim Yim25% (4)
- Bio 320 Practical 7Dokumen12 halamanBio 320 Practical 7MuhammadAsyraf50% (2)
- 76) Book Chapter 2010Dokumen11 halaman76) Book Chapter 2010Giovanni MauroBelum ada peringkat
- The Pathophysiology of AmenorrheaDokumen6 halamanThe Pathophysiology of AmenorrheaTri Suci UtamiBelum ada peringkat
- Rubins-Q A ENDOCRINEDokumen14 halamanRubins-Q A ENDOCRINECRUZ Jill EraBelum ada peringkat
- Module 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionDokumen229 halamanModule 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionA.h.MuradBelum ada peringkat
- Drug StudyDokumen14 halamanDrug StudyTin BernardezBelum ada peringkat
- MicronutrientsDokumen21 halamanMicronutrientsJohn Paolo OcampoBelum ada peringkat
- 8.sadvritta (Code of Conduct)Dokumen47 halaman8.sadvritta (Code of Conduct)Vanisha AnoepBelum ada peringkat
- Buteyko Breathing ExercisesDokumen5 halamanButeyko Breathing ExercisesjoseBelum ada peringkat
- Dirty Genes Course Copy 1Dokumen181 halamanDirty Genes Course Copy 1Rachel Bruce50% (4)
- CVP Insertion Close Tube Thoracostomy RDokumen6 halamanCVP Insertion Close Tube Thoracostomy RFaye Nadine T. CABURALBelum ada peringkat
- Intrinsic RBC DisordersDokumen4 halamanIntrinsic RBC DisordersMartin ClydeBelum ada peringkat
- Nursing DictionaryDokumen353 halamanNursing DictionaryEmmanuel BoadBelum ada peringkat
- Amphibian Graphs?Dokumen9 halamanAmphibian Graphs?Anshumaan PatraBelum ada peringkat