Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hand Injuries EditedDokumen25 halamanHand Injuries EditedSurgicalgownBelum ada peringkat
- Rapid Sequence Ion EditedDokumen52 halamanRapid Sequence Ion EditedSurgicalgownBelum ada peringkat
- Acute Low Back Pain EditedDokumen35 halamanAcute Low Back Pain EditedSurgicalgownBelum ada peringkat
- Peripartum Cardiomyopathy: Adapted From SourceDokumen37 halamanPeripartum Cardiomyopathy: Adapted From SourceSurgicalgownBelum ada peringkat
- Fractures of Shoulder and Elbow EditedDokumen25 halamanFractures of Shoulder and Elbow EditedSurgicalgownBelum ada peringkat
- Stroke Management: Adapted From SourceDokumen53 halamanStroke Management: Adapted From SourceSurgicalgownBelum ada peringkat
- Management Head and Neck Cancer EditedDokumen45 halamanManagement Head and Neck Cancer EditedSurgicalgownBelum ada peringkat
- Dental Emergencies EditedDokumen41 halamanDental Emergencies EditedSurgicalgownBelum ada peringkat
- Violence in The ER EditedDokumen40 halamanViolence in The ER EditedSurgicalgownBelum ada peringkat
- Toxidromes EditedDokumen11 halamanToxidromes EditedSurgicalgownBelum ada peringkat
- Asthma VPL 2 EditedDokumen39 halamanAsthma VPL 2 EditedSurgicalgownBelum ada peringkat
- Eye Trauma: Penetrating and BluntDokumen68 halamanEye Trauma: Penetrating and BluntSurgicalgownBelum ada peringkat
- Pulmonary Embolism As Seen in The ED EditedDokumen40 halamanPulmonary Embolism As Seen in The ED EditedSurgicalgownBelum ada peringkat
- Meningitis Adapted From SourceDokumen26 halamanMeningitis Adapted From SourceSurgicalgownBelum ada peringkat
- Head Injury Management EditedDokumen49 halamanHead Injury Management EditedSurgicalgownBelum ada peringkat
- Hyper Kale Mia EditedDokumen63 halamanHyper Kale Mia EditedSurgicalgownBelum ada peringkat
- Hypothermia: - Adapted From SourceDokumen21 halamanHypothermia: - Adapted From SourceSurgicalgownBelum ada peringkat
- Envenom at Ion EditedDokumen74 halamanEnvenom at Ion EditedSurgicalgownBelum ada peringkat
- How To Read CXR EditedDokumen66 halamanHow To Read CXR EditedSurgicalgownBelum ada peringkat
- Chestpain How To Treat EditedDokumen45 halamanChestpain How To Treat EditedSurgicalgownBelum ada peringkat
- Asthma EditedDokumen42 halamanAsthma EditedSurgicalgownBelum ada peringkat
- Acute Bronchiolitis EditedDokumen19 halamanAcute Bronchiolitis EditedSurgicalgownBelum ada peringkat
- Acute Coronary Syndrome EditedDokumen38 halamanAcute Coronary Syndrome EditedSurgicalgownBelum ada peringkat
- Abdominal Pain - EditedDokumen48 halamanAbdominal Pain - EditedSurgicalgownBelum ada peringkat
- Commercialization of Medical Intellectual PropertyDokumen5 halamanCommercialization of Medical Intellectual PropertySurgicalgown100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Ankylosing SpondylitisDokumen24 halamanAnkylosing SpondylitisSiva ShanmugamBelum ada peringkat
- Lastexception 63783215917Dokumen12 halamanLastexception 63783215917Rey valdyBelum ada peringkat
- Cygnet Sea Dragons Junior Soccer Club - Saturday 18 MayDokumen27 halamanCygnet Sea Dragons Junior Soccer Club - Saturday 18 MayDave SayersBelum ada peringkat
- Hema Control Reference RangeDokumen19 halamanHema Control Reference Rangeclarisse salvadorBelum ada peringkat
- McLaren 750S Spider Order A8LCK24 Summary 2023-11-05Dokumen6 halamanMcLaren 750S Spider Order A8LCK24 Summary 2023-11-05Ahmad Al-abdulghaniBelum ada peringkat
- Despiece Megelli 125 RDokumen22 halamanDespiece Megelli 125 RAlfredo Rosselli100% (2)
- Zru Newsletter 4Dokumen4 halamanZru Newsletter 4Grant Peter MitchellBelum ada peringkat
- Ork HuntersDokumen1 halamanOrk Huntersjnppapa5484Belum ada peringkat
- CPCD 547998Dokumen911 halamanCPCD 547998manuel eduardo pomahuali liñanBelum ada peringkat
- FIFA World Cup™ Trophy Tour by Coca-ColaDokumen2 halamanFIFA World Cup™ Trophy Tour by Coca-ColapdmrrBelum ada peringkat
- Paper C 2019Dokumen22 halamanPaper C 2019Minh Bui0% (1)
- Thư ITECOM - License of Netnumen of ContractDokumen3 halamanThư ITECOM - License of Netnumen of ContractDung (David) Nguyen CongBelum ada peringkat
- Biotechnology Reviewer - Photosynthesis and Cellular RespirationDokumen3 halamanBiotechnology Reviewer - Photosynthesis and Cellular RespirationMaribeth VillanuevaBelum ada peringkat
- Bangsbo, Iaia, Krustrup - 2008 - The Yo-Yo Intermittent Recovery Test A Useful Tool For Evaluation of Physical Performance in IntermitteDokumen16 halamanBangsbo, Iaia, Krustrup - 2008 - The Yo-Yo Intermittent Recovery Test A Useful Tool For Evaluation of Physical Performance in Intermittemateus.santosBelum ada peringkat
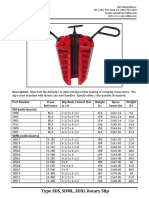
- Type SDS SDML SDXL Rotary Slip Cut SheetDokumen2 halamanType SDS SDML SDXL Rotary Slip Cut SheetJose Barrero100% (1)
- A School NewsletterDokumen4 halamanA School NewslettererinconradBelum ada peringkat
- Lista de Artículos Disponibles 27-Agosto-18 Devir MéxicoDokumen60 halamanLista de Artículos Disponibles 27-Agosto-18 Devir MéxicoSigfridoOrgridBelum ada peringkat
- D3 USL Pitch DeckDokumen31 halamanD3 USL Pitch DeckfidouBelum ada peringkat
- Prepare To Pass VideosDokumen13 halamanPrepare To Pass VideosImran Mobin100% (1)
- Chess Life - 2022 - 8Dokumen68 halamanChess Life - 2022 - 8Dusty KramerBelum ada peringkat
- Exercise: Cristina M. Medina, RN, MAN Jayme P. Hipolito, RN, MAN Lorna Mendoza, RN, MANDokumen26 halamanExercise: Cristina M. Medina, RN, MAN Jayme P. Hipolito, RN, MAN Lorna Mendoza, RN, MANAlma Janella TOSINOBelum ada peringkat
- MCD Slb801 enDokumen4 halamanMCD Slb801 endino_pBelum ada peringkat
- Trolleybus Model 42003 Two-AxleDokumen2 halamanTrolleybus Model 42003 Two-AxleRodrigo SampaioBelum ada peringkat
- ProductsHarrington CF Hand Chain Hoist - To 5 TonDokumen4 halamanProductsHarrington CF Hand Chain Hoist - To 5 TonSapriyun SBelum ada peringkat
- Datasheet Kent C 0126 PDFDokumen2 halamanDatasheet Kent C 0126 PDFFWEFWEFWBelum ada peringkat
- klf300 c15 c17 Parts List PDFDokumen97 halamanklf300 c15 c17 Parts List PDFOliverBelum ada peringkat
- Grab Start TranslateDokumen2 halamanGrab Start TranslateSatria WibowoBelum ada peringkat
- 05 PPT LubeDokumen36 halaman05 PPT LubeFajar DP100% (1)
- Long JumpDokumen10 halamanLong JumpAdi JaatBelum ada peringkat
- VariantsDokumen4 halamanVariantsJESUSBelum ada peringkat